Aug 07, 2025
Simulation of MR-Guided Focused Ultrasound for Cervical Facet Joint Ablation Using MRI and CT-Based Anatomical Models
- Marta M. Iversen1,
- Michelle Kline2,
- Emily A. Smith3,
- Allison Payne2,
- Lubdha M. Shah2,4,
- Viola Rieke2
- 1University of Utah, Department of Physical Medicine and Rehabilitation;
- 2University of Utah, Department of Radiology and Imaging Sciences;
- 3University of Utah, Department of Biomedical Engineering;
- 4University of Utah Department of Neurosurgery
- SPARCTech. support email: [email protected]



External link: http://doi:10.1080/02656736.2025.2500487
Protocol Citation: Marta M. Iversen, Michelle Kline, Emily A. Smith, Allison Payne, Lubdha M. Shah, Viola Rieke 2025. Simulation of MR-Guided Focused Ultrasound for Cervical Facet Joint Ablation Using MRI and CT-Based Anatomical Models. protocols.io https://dx.doi.org/10.17504/protocols.io.5jyl8wxk6l2w/v1
Manuscript citation:
Iversen MM, Kline M, Smith EA, Payne A, Shah LM, Rieke V. Ablation of cervical facet joints is safe and feasible with two magnetic resonance-guided focused ultrasound transducers as demonstrated by thermal simulations. Int J Hyperthermia. 2025; 41. doi:10.1080/02656736.2025.2500487
License: This is an open access protocol distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Protocol status: Working
We use this protocol and it's working
Created: April 28, 2025
Last Modified: August 07, 2025
Protocol Integer ID: 189852
Keywords: cervical spine, MRI, CT, simulation, FUS, MRgFUS, focused ultrasound, facet joint, guided focused ultrasound for cervical facet joint ablation, guided focused ultrasound, cervical facet joint ablation, focused ultrasound, focused ultrasound transducer type, cervical facet joint, treatments to cervical facet joint, ultrasound transducer type, simulation of mr, using mri, multiple cervical level, simulating mr, based anatomical model, imaging acquisition, resolution mri, tissue response, anatomical models this protocol
Funders Acknowledgements:
NIH Heal Initiative
Grant ID: U18 EB030607
NIH
Grant ID: UH3 AR076736
Abstract
This protocol outlines the methods for simulating MR-guided focused ultrasound (MRgFUS) treatments to cervical facet joints using high-resolution MRI and CT data. It includes imaging acquisition, segmentation, acoustic and thermal simulation, and safety analysis using two focused ultrasound transducer types. Tissue response to focused ultrasound was modeled and evaluated across multiple cervical levels and beam angles to assess feasibility and safety.
Materials
| Equipment | Specifications | |
| MRI Scanner | 3T (MAGNETOM Skyra/Vida) or 1.5T (MAGNETOM Aera), Siemens | |
| CT Scanner | Clinical CT system with cervical spine protocol | |
| Segmentation Software | Seg3D | |
| Simulation Tools | HAS algorithm and finite difference solver for Pennes bioheat equation | |
| Tissue Property Database | IT’IS Foundation Tissue Properties (acoustic and thermal) |
Before start
Ensure IRB approval for retrospective use of clinical imaging data.
Participant Selection and Imaging
We simulated ultrasound treatments in the necks of six individuals. Participants included four patients referred for general neck imaging and two healthy volunteers. Imaging was performed on either a 3T (MAGNETOM Skyra or Vida) or 1.5T (MAGNETOM Aera) Siemens scanner.
3T Imaging Parameters:
- Gradient echo
- TR = 6.68 ms
- TE = 2.46 ms (in phase), 3.69 ms (out of phase)
- Echo train length = 2
- 1 average
1.5T Imaging Parameters:
- Gradient echo
- TR = 6.97 ms
- TE = 2.39 ms (in phase), 4.47 ms (out of phase)
- Echo train length = 2
- 4 averages
Axial T1 Dixon sequences were used for visualizing fat and muscle. Zero-filling was applied to achieve 0.5 mm isotropic resolution. All imaging was IRB-approved.
CT-Based Anatomical Measurement
We analyzed cervical spine CTs from 40 individuals for planning transducer reach.
Measurements included:
- Depth from skin to each facet joint target (0-degree angle)
- Distance between left and right targets
Treatment Strategy and Scope
We simulated treatment at all cervical levels bilaterally, assuming mechanical transducer motion between angles of 0–30° in the axial plane. Simulations investigated safety of targeting facet joints at 0°, 15°, and 30° using FUS.
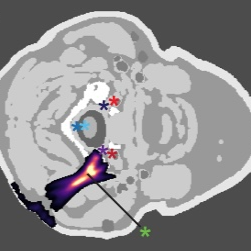
Target and Off-Target Locations
Facet joints from C2-3 to C6-7 were manually identified by a neuroradiologist on MR images. Off-target structures included spinal nerves, the spinal cord, and major arteries (vertebral, carotid).
Segmentation Methods
Seg3D was used to segment MRI into 8 tissue types: water, CSF, vessels, fat, muscle, skin, bone, spinal cord.
- Non-skin layers: thresholding → manual correction → isolation (Boolean
Remove)
- Skin layer: smoothed dilation/erosion on all-tissue mask + Boolean Remove
Ultrasound Simulations
We used the Hybrid-Angular Spectrum (HAS) method to simulate ultrasound propagation. Transducers were modeled using the Rayleigh-Sommerfeld integral. Tissue acoustic properties were from the IT’IS Foundation database.
Each model underwent 60 simulations (5 cervical levels, 2 sides, 3 angles, 2 transducers). Output was 3D pressure and power deposition. Nonlinear effects were ignored (P < 5 MPa).
Thermal Simulations
Thermal effects were modeled using the Pennes bioheat equation with 100 W ultrasound power. Assumptions:
- Boundary temperature = 37°C
- Tissue perfusion effects modeled for blood vessels
Pennes bioheat equation
Thermaldose (CEM 43°C) calculated over 20 s sonication and 60 s cooling using:
(R= 2 if T≥43°C; R = 4 if T<43°C)
Code for simulations: GitHub
Tissue Ablation and Safety
Ablation target: 60°C or >240 CEM.
Transducers
Transducer S11: 256-element, symmetric, 1 MHz, 11 cm focal length
Transducer A10: 256-element, asymmetric, 1 MHz, 10 cm focal length
Transducer Comparison
Free-field tests showed S11 produced 120.7% higher peak pressure (4.7 MPa) vs A10 (3.9 MPa). Simulations recorded:
- Peak temp at target
- Mean temp in 10 mm ROI
- Temp at off-target sites
Statistical tests:
- Normality: Anderson-Darling
- Significance: Wilcoxon signed-rank (only ΔT > 5°C tested)
Protocol references
Vyas, U. & Christensen, D. Ultrasound beam simulations in inhomogeneous tissue geometries using the hybrid
angular spectrum method. IEEE Transactions on Ultrasonics, Ferroelectrics, and Frequency Control 59, 1093–1100 (2012).
Hasgall, P. et al. IT’IS Database for thermal and electromagnetic parameters of biological tissues. https://doi.org/10.13099/VIP21000-04-1 (2022).
Dillon, C. R., Payne, A., Christensen, D. A. & Roemer, R. B. The accuracy and precision of two non-invasive, magnetic resonance-guided focused ultrasound-based thermal diffusivity estimation methods. Int J Hyperthermia30, 362–371 (2014).
Dillon, C. R., Vyas, U., Payne, A., Christensen, D. A. & Roemer, R. B. An analytical solution for improved HIFU SAR estimation. Phys Med Biol 57, 4527–4544 (2012).
Sapareto, S. A. & Dewey, W. C. Thermal dose determination in cancer therapy. Int J Radiat Oncol Biol Phys 10, 787–800 (1984).