Sep 29, 2025
Protocol for performing total hip arthroplasty without admission to the ICU

- Berliet Assad1,
- Fabrício Bolpato Loures1,
- Gustavo Perisse1,
- Marcelo Kokis1,
- Luciana Xavier1,
- Bruno Rabelo1,
- Liszt Palmeira de Oliveira1
- 1Universidade do Estado do Rio de Janeiro (UERJ)
- Liszt Palmeira de Oliveira: Head of the orthopedics service at UERJ



Protocol Citation: Berliet Assad, Fabrício Bolpato Loures, Gustavo Perisse, Marcelo Kokis, Luciana Xavier, Bruno Rabelo, Liszt Palmeira de Oliveira 2025. Protocol for performing total hip arthroplasty without admission to the ICU. protocols.io https://dx.doi.org/10.17504/protocols.io.14egnrm4yl5d/v1
License: This is an open access protocol distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Protocol status: In development
We are still developing and optimizing this protocol
Created: September 19, 2025
Last Modified: September 29, 2025
Protocol Integer ID: 227751
Keywords: Hip, Arthroplasty , Intensive care unit , icu total hip arthroplasty, total hip arthroplasty without postoperative admission, total hip arthroplasty without admission, performing total hip arthroplasty, postoperative admission, effective surgery, compromising patient safety, elderly patient, clinical criteria, patient safety
Abstract
Total hip arthroplasty is a safe and effective surgery, however large and aimed at elderly patients. The objective of this protocol is to define clinical criteria for performing total hip arthroplasty without postoperative admission to the ICU, without compromising patient safety.
Attachments
Guidelines
Protocol based on review of current medical literature
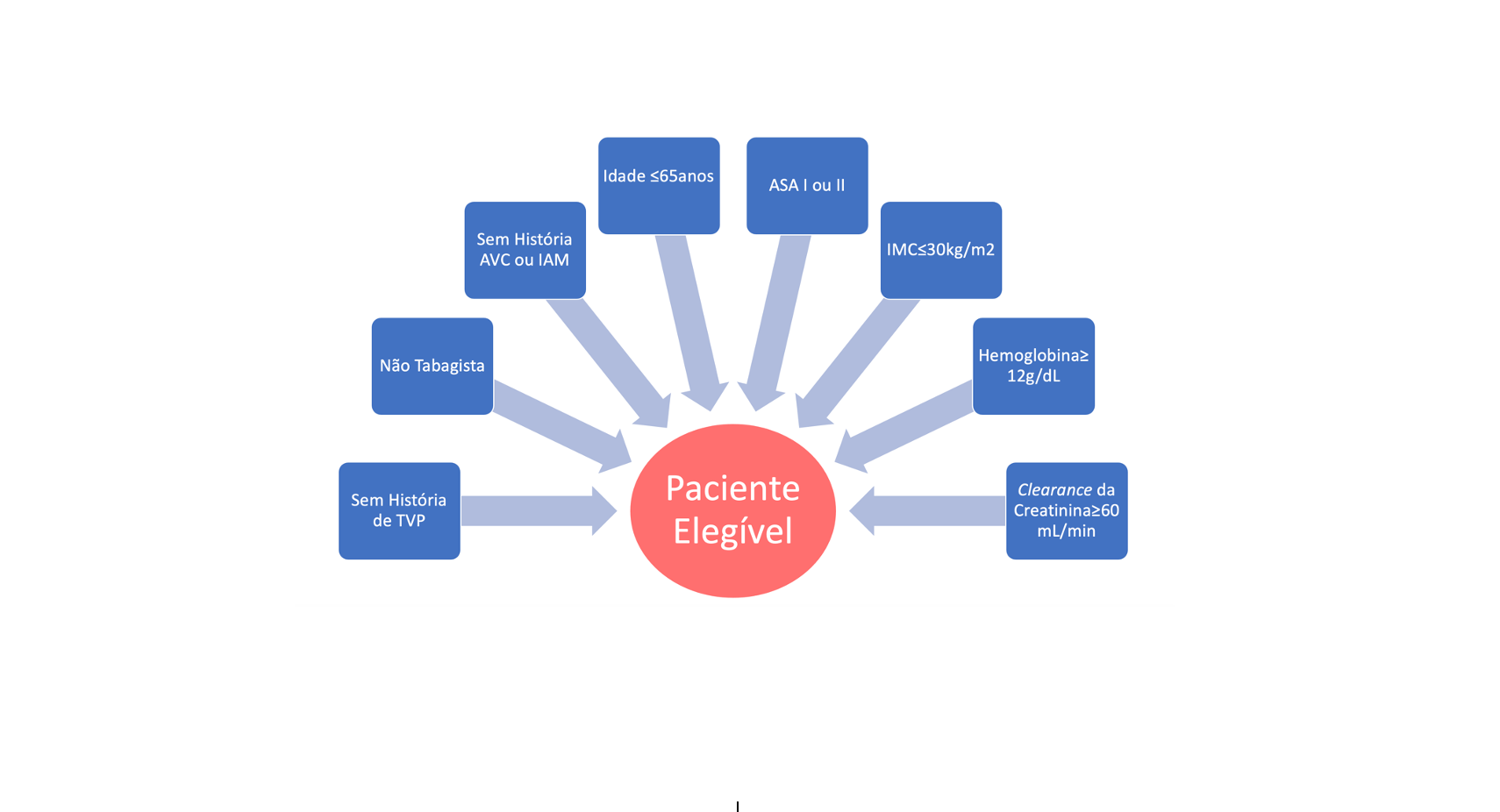
To perform total hip arthroplasty, without the need to reserve an ICU and without compromising patient safety, the following clinical criteria must be followed:
1- Less than 65 years old
2- American Society Anesthesiology (ASA) Classification I or II
3- Non-smoker
4- No history of ischemic disease (Acute Myocardial Infarction
and/or Cerebrovascular disease)
5- No history of deep vein thrombosis
7- BMI less than 30kg/m2
8- Creatinine clearance higher than 60 ml/min
9- Hemoglobin higher than 12g/dL
Safety warnings
Similar protocols have proven to be safe and effective
Before start
Before start, it is important to carry out a multidisciplinary assessment of the patient and review the epidemiological profile of your institution.
Protocol references
1- Loures FB, Góes RFA, Gusmão CV, Albuquerque RSPE, Labronici PJ. Epidemiological and Clinical Profile of Patients Submitted to Total Knee Arthroplasty.
Rev Bras Ortop (Sao Paulo). 2021;57(2):223-229. doi: 10.1055/s-0041-1724080
2- Loures F, Reis JH, Campos MO, Runco GM, Fonseca LDV, Xavier LF, et al.
Criteria for performing total knee arthroplasty without postoperative intensive care monitoring. protocols.io. 2022. doi: dx.doi.org/10.17504/protocols.
io.bp2l6b325gqe/v2.
3- Liodakis E, Bergeron SG, Zukor DJ, Huk OL, Epure LM, Antoniou J. Perioperative
Complications and Length of Stay After Revision Total Hip and Knee Arthroplasties: An Analysis of the NSQIP Database. J Arthroplasty. 2015;30(11):1868-71.
doi: 10.1016/j.arth.2015.05.029.
4- Tischler EH, Matsen Ko L, Chen AF, Maltenfort MG, Schroeder J, Austin MS.
Smoking Increases the Rate of Reoperation for Infection within 90 Days After
Primary Total Joint Arthroplasty. J Bone Joint Surg Am. 2017;99(4):295-304.
doi: 10.2106/JBJS.16.00311.
5- AbdelSalam H, Restrepo C, Tarity TD, Sangster W, Parvizi J. Predictors of
intensive care unit admission after total joint arthroplasty. J Arthroplasty.
2012;27(5):720-5. doi: 10.1016/j.arth.2011.09.027.
6- Kuperman EF, Schweizer M, Joy P, Gu X, Fang MM. The effects of advanced on primary total knee arthroplasty: a meta-analysis and systematic review.
BMC Geriatr. 2016;16:41. doi: 10.1186/s12877-016-0215-4.
7- Klausing A, Martini M, Wimmer MD, Gravius S, Wirtz DC, Randau TM. Postoperative Medical Complications and Intermediate Care Unit/Intensive Care
Unit Admission in Joint Replacement Surgery: A Prospective Risk Model. J
Arthroplasty. 2019;34(4):717-722. doi: 10.1016/j.arth.2018.12.034.
8- Bjorgul K, Novicoff WM, Saleh KJ. Evaluating comorbidities in total hip and knee
arthroplasty: available instruments. J Orthop Traumatol. 2010;11(4):203-9. doi:
10.1007/s10195-010-0115-x