Dec 14, 2024
NCI Biospecimen Evidence-Based Practices (BEBP) - Snap-freezing of Post-Surgical Tissue Biospecimens
- NCI Biorepositories and Biospecimen Research Branch1
- 1National Cancer Institute


External link: https://biospecimens.cancer.gov/resources/bebp.asp
Protocol Citation: NCI Biorepositories and Biospecimen Research Branch 2024. NCI Biospecimen Evidence-Based Practices (BEBP) - Snap-freezing of Post-Surgical Tissue Biospecimens. protocols.io https://dx.doi.org/10.17504/protocols.io.5jyl825zrl2w/v1
Manuscript citation:
Engel KB, Vaught JM, Moore HM. (2014). National Cancer Institute Biospecimen Evidence-Based Practices: A novel approach to pre-analytical standardization. Biopreservation and Biobanking. 12(2): 148-50. PMID 24749882.
License: This is an open access protocol distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Protocol status: Working
This document contains guidance that is intended to facilitate the development of evidence-based standard operating procedures.
Created: April 29, 2024
Last Modified: December 14, 2024
Protocol Integer ID: 98952
Keywords: snap-freezing, tissue, liquid nitrogen, specimen handling, preservation, storage, NCI, BEBP, evidence-based, nci biospecimen evidence, biospecimen, applicable to all human tissue, primary tissue culture, use as donor specimen, human tissue, donor specimen
Disclaimer
This document contains guidance that is intended to facilitate the development of evidence-based standard operating procedures.
Abstract
This evidence-based best practice document is applicable to all human tissues that are to be preserved by snap-freezing. Biospecimens preserved under these procedural guidelines are suitable for downstream analysis of DNA, RNA, protein, and morphology endpoints. Additional analytical endpoints, including but not limited to cell viability, cell sorting, drug sensitivity testing, or use as donor specimens for xenografts or primary tissue culture, do not fall within the scope of this document.
Attachments

Guidelines
9.1.1. Universal Precautions (CDC, 1987):
http://www.cdc.gov/mmwr/preview/mmwrhtml/00000039.htm; Tools for Protecting Healthcare Personnel, CDC: http://www.cdc.gov/HAI/prevent/ppe.html.
9.1.2. CLSI IL-28A: Quality Assurance for Design Control and Implementation of Immunohistochemistry Assays; Approved Guideline—Second Edition. S Hewitt, personal communications, draft CLSI IL-28a.
9.1.3. CLSI MM13-A: Collection, Transport, Preparation, and Storage of Specimens for Molecular Methods; Approved Guideline. 2008. Vol25, No 31.
9.1.4. Mager SR, Oomen MH, Morente MM, Ratcliffe C, Knox K, Kerr DJ, Pezzella F, Riegman PH: Standard operating procedure for the collection of fresh frozen tissue samples. Eur J Cancer 2007, 43(5):828-834.
9.1.5. Morente MM, Mager R, Alonso S, Pezzella F, Spatz A, Knox K, Kerr D, Dinjens WN, Oosterhuis JW, Lam KH et al: TuBaFrost 2: Standardising tissue collection and quality control procedures for a European virtual
frozen tissue bank network. Eur J Cancer 2006, 42(16):2684-2691.
Materials
5.1. Plastic-backed absorbent bench paper.
5.2. New disposable dissecting equipment for each organ.
5.3. Liquid Nitrogen (LN2).
5.4. Dewar flask.
5.5. Cryogenic specimen storage container (cryovial, cryostraw, cryosette‱, cryomold, or equivalent storage container designed for temperatures at or below -190°C), LN2 storage container or, in the event of immediate shipment, LN2 dry shipper.
5.6. Should LN2 be unavailable, alternative freezing media may include: isopentane pre-cooled with LN2; isopentane cooled with dry ice; dry ice alone; -80°C freezer. When utilizing dry ice or -80°C for freezing and storing at -80°C, suitable cryogenic specimen storage containers designed for temperatures at or below -80°C will be acceptable and shipment may be performed on dry ice.
Troubleshooting
Safety warnings
Universal Precautions (CDC-1978) are used for all phases of organ/tissue dissection and handling (See Reference 9.1.1).
Ethics statement
Protocols developed using this Biospecimen Evidence-Based Practice may require approval by the user’s institutional review board (IRB) or an equivalent ethics committee prior to implementation.
Before start
The purpose of this document is to provide evidence-based guidance for the proper snap-freezing of human tissue biospecimens. This guidance is intended to support the development and execution of evidence-based Standard Operating Procedures (SOPs) for human biospecimen collection, processing, and storage operations.
Recording of biospecimen preacquistion data
Whenever possible, extensive data should be recorded relating to preacquisition conditions that may affect the integrity of the biospecimen. Such data may include patient information (including age, gender, diagnosis, and treatment) as well as details relating to surgery and biospecimen acquisition (including the use of anesthesia, warm ischemia time, and surgical procedure and duration).
Preparation of freezing containers and bench space
Pre-labeled cryogenic specimen storage containers for each organ being dissected should be identified and arranged before the organ is available for dissection.
Specimen containers should be appropriately labeled and organized, and tissues of different anatomic sites as well as tumor and normal tissues should be segregated to the extent possible.
Clean disposable scalpels and forceps should be used when cutting different tissue types of the same patient and specimens from different patients. Contact with absorbent materials that may contaminate dissected research tissues or where capillary action may draw fluid from tissue samples should be avoided.
Post-collection storage of tissue specimens on wet ice
Specimens may be placed in a sterile closed container on On ice until dissection (See Section 8.1 in the Attached PDF for Literature Evidence).
Minimizing cold ischemia time
Dissection should be accomplished soon after the specimen is released by the supervising physician. Cold ischemia time should be minimized as much as possible, optimally less than 20 min but no more than 01:00:00 (See Section 8.2 in the Attached PDF for Literature Evidence). Cold ischemia time should be documented for every module or segment and for each subsequent aliquot.
For tissue specimens collected postmortem, postmortem interval (PMI) should be minimized as much as possible, optimally less than 2 hours, but no more than 6 h (See Section 8.3 in the Attached PDF for Literature Evidence). This time should be documented for every patient and attached to the module and its aliquots.
Dissection notes
Dissection should be performed one organ at a time. Final aliquots should be no thicker than0.4 cm and placed into the proper cryogenic specimen storage containers. If morphological analysis is anticipated, then specimens can be surrounded by Optimal Cutting Temperature (OCT) Compound prior to freezing; however, the use of OCT Compound is not optimal for some specific molecular analysis methods (See Section 8.4 in the Attached PDF for Literature Evidence).
Freezing of tissues
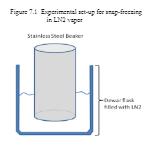
Optimally, the tightly sealed cryogenic specimen storage container should be frozen in liquid nitrogen (LN2) vapor. This can be achieved by suspending a stainless steel beaker inside a bench top Dewar flask pre-filled with LN2 (See Figure 7.1 in the Attached PDF). The specimen storage container should then be placed inside the steel beaker for 00:02:00 or less depending on the size of the specimen (See Section 8.5 in the Attached PDF for Literature Evidence). Common alternatives to freezing in LN2 vapor may include freezing by immersion in LN2 or immersion in isopentane precooked to -80 °C or below (See Section 8.6 in the Attached PDF for Literature Evidence).
If LN2 is unavailable at the physical site where specimens are collected and preserved, alternative freezing methods may used, and include immersion in isopentane pre-cooled with dry ice, placement on dry ice, or placement in a -80 °C freezer. Freezing specimens directly on dry ice should be avoided if they are to be used for morphological analysis (See Section 8.7 in the Attached PDF for Literature Evidence).
Transfer and storage of frozen biospecimens
After freezing, the cryogenic specimen storage container should be transferred for storage in an LN2 vapor freezer. Should LN2 be unavailable, specimen storage containers may be stored at -70 °C or colder (See Section 8.8 in the Attached PDF for Literature Evidence).
Alternatively, the frozen specimens may be placed directly into an LN2 dry shipper for immediate transport (See Section 8.8 in the Attached PDF for Literature Evidence). Specimen containers frozen in LN2 and destined for storage in LN2 should be held in LN2 vapor before and during transfer to repository/long-term storage. Should LN2 be unavailable, specimen storage containers may be shipped on dry ice.
Specimen containers destined for storage at -80 °C should be held on dry ice before and during transport.
Protocol references
References considered during the development of this NCI BEBP document are listed below (also See Section 9.2 in the Attached PDF) and include hyperlinks to the PubMed abstract and NCI Biospecimen Research Database curation where applicable. References are cited within the Summaries of Literature Evidence (See Section 7.0) in the Attached PDF.
1. Micke, P., et al., Biobanking of fresh frozen tissue: RNA is stable in nonfixed surgical specimens. Lab Invest, 2006. 86(2): p. 202-11.
2. van Maldegem, F., et al., Effects of processing delay, formalin fixation, and immunohistochemistry on RNA Recovery From Formalin-fixed Paraffin-embedded Tissue Sections. Diagn Mol Pathol, 2008. 17(1): p. 51-8.
3. Hůlková, M. and J. Zeman, Placental tissue as model for pilot study focused on RNA analysis from human foetal tissue. Prague Med Rep, 2011. 112(2): p. 93-101.
4. Espina, V., et al., A portrait of tissue phosphoprotein stability in the clinical tissue procurement process. Mol Cell Proteomics, 2008. 7(10): p. 1998-2018.
5. Walker, L.A., et al., Tissue procurement strategies affect the protein biochemistry of human heart samples. J Muscle Res Cell Motil, 2011. 31(5-6): p. 309-14.
6. Huang, J., et al., Effects of ischemia on gene expression. J Surg Res, 2001. 99(2): p. 222-7.
7. Spruessel, A., et al., Tissue ischemia time affects gene and protein expression patterns within minutes following surgical tumor excision. Biotechniques, 2004. 36(6): p. 1030-7.
8. Bray, S.E., et al., Gene expression in colorectal neoplasia: modifications induced by tissue ischaemic time and tissue handling protocol. Histopathology, 2010. 56(2): p. 240-50.
9. Johnsen, I.K., et al., Evaluation of a standardized protocol for processing adrenal tumor samples: preparation for a European adrenal tumor bank. Horm Metab Res, 2010. 42(2): p. 93-101.
10. Jones, R.J., et al., The impact of delay in cryo-fixation on biomarkers of Src tyrosine kinase activity in human breast and bladder cancers. Cancer Chemother Pharmacol, 2008. 61(1): p. 23-32.
11. De Cecco, L., et al., Impact of biospecimens handling on biomarker research in breast cancer. BMC Cancer, 2009. 9: p. 409.
12. Blackhall, F.H., et al., Stability and heterogeneity of expression profiles in lung cancer specimens harvested following surgical resection. Neoplasia, 2004. 6(6): p. 761-7.
13. Sehringer, B., et al., Evaluation of different strategies for real-time RT-PCR expression analysis of corticotropin-releasing hormone and related proteins in human gestational tissues. Anal Bioanal Chem, 2005. 383(5): p. 768-75.
14. Jewell, S.D., et al., Analysis of the molecular quality of human tissues: an experience from the Cooperative Human Tissue Network. Am J Clin Pathol, 2002. 118(5): p. 733-41.
15. Hatzis, C., et al., Effects of tissue handling on RNA integrity and microarray measurements from resected breast cancers. J Natl Cancer Inst, 2011. 103(24): p. 1871-83.
16. Sewart, S., et al., Molecular analysis of a collection of clinical specimens stored at 4 degrees C as an alternative to snap-freezing. Int J Oncol, 2009. 35(2): p. 381-6.
17. Bergers, E., et al., The influence of fixation delay on mitotic activity and flow cytometric cell cycle variables. Hum Pathol, 1997. 28(1): p. 95-100.
18. Viana, C.R., et al., The interference of cold ischemia time in the quality of total RNA from frozen tumor samples. Cell Tissue Bank, 2012.
19. Freidin, M.B., et al., Impact of collection and storage of lung tumor tissue on whole genome expression profiling. J Mol Diagn, 2012. 14(2): p. 140-8.
20. Bao, W.G., et al., Biobanking of Fresh-frozen Human Colon Tissues: Impact of Tissue Ex-vivo Ischemia Times and Storage Periods on RNA Quality. Ann Surg Oncol, 2012.
21. Bertilsson, H., et al., RNA quality in fresh frozen prostate tissue from patients operated with radical prostatectomy. Scand J Clin Lab Invest, 2010. 70(1): p. 45-53.
22. Copois, V., et al., Impact of RNA degradation on gene expression profiles: assessment of different methods to reliably determine RNA quality. J Biotechnol, 2007. 127(4): p. 549-59.
23. Strand, C., et al., RNA quality in frozen breast cancer samples and the influence on gene expression analysis--a comparison of three evaluation methods using microcapillary electrophoresis traces. BMC Mol Biol, 2007. 8: p. 38.
24. Naber, D. and H.G. Dahnke, Protein and nucleic acid content in the aging human brain. Neuropathol Appl Neurobiol, 1979. 5(1): p. 17-24.
25. Preece, P., et al., An optimistic view for quantifying mRNA in post-mortem human brain. Brain Res Mol Brain Res, 2003. 116(1-2): p. 7-16.
26. Preece, P. and N.J. Cairns, Quantifying mRNA in postmortem human brain: influence of gender, age at death, postmortem interval, brain pH, agonal state and inter-lobe mRNA variance. Brain Res Mol Brain Res, 2003. 118(1-2): p. 60-71.
27. Kobayashi, H., et al., Stability of messenger RNA in postmortem human brains and construction of human brain cDNA libraries. J Mol Neurosci, 1990. 2(1): p. 29-34.
28. De Paepe, M.E., et al., Postmortem RNA and protein stability in perinatal human lungs. Diagn Mol Pathol, 2002. 11(3): p. 170-6.
29. Birdsill, A.C., et al., Postmortem interval effect on RNA and gene expression in human brain tissue. Cell Tissue Bank, 2011. 12(4): p. 311-8.
30. Heinrich, M., et al., Successful RNA extraction from various human postmortem tissues. Int J Legal Med, 2007. 121(2): p. 136-42.
31. Johnson, S.A., D.G. Morgan, and C.E. Finch, Extensive postmortem stability of RNA from rat and human brain. J Neurosci Res, 1986. 16(1): p. 267-80.
32. Cummings, T.J., et al., Recovery and expression of messenger RNA from postmortem human brain tissue. Mod Pathol, 2001. 14(11): p. 1157-61.
33. Atz, M., et al., Methodological considerations for gene expression profiling of human brain. J Neurosci Methods, 2007. 163(2): p. 295-309.
34. Schramm, M., et al., Stability of RNA transcripts in post-mortem psychiatric brains. J Neural Transm, 1999. 106(3-4): p. 329-35.
35. Sherwood, K.R., et al., RNA integrity in post mortem human variant Creutzfeldt-Jakob disease (vCJD) and control brain tissue. Neuropathol Appl Neurobiol, 2011. 37(6): p. 633-42.
36. Larsen, S., et al., Northern and Southern blot analysis of human RNA and DNA in autopsy material. APMIS, 1992. 100(6): p. 498-502.
37. Gala, J.L., et al., HIV-1 detection by nested PCR and viral culture in fresh or cryopreserved postmortem skin: potential implications for skin handling and allografting. J Clin Pathol, 1997. 50(6): p. 481-4.
38. Goggins, M., J.M. Scott, and D.G. Weir, Regional differences in protein carboxymethylation in post-mortem human brain. Clin Sci (Lond), 1998. 94(6): p. 677-85.
39. Steu, S., et al., A procedure for tissue freezing and processing applicable to both intra-operative frozen section diagnosis and tissue banking in surgical pathology. Virchows Arch, 2008. 452(3): p. 305-12.
40. Turbett, G.R. and L.N. Sellner, The use of optimal cutting temperature compound can inhibit amplification by polymerase chain reaction. Diagn Mol Pathol, 1997. 6(5): p. 298-303.
41. Pasic, R., B. Djulbegovic, and J.L. Wittliff, Influence of O.C.T. embedding compound on determinations of estrogen and progestin receptors in breast cancer. Clin Chem, 1989. 35(12): p. 2317-9.
42. Muensch, H. and W.C. Maslow, Interference of O.C.T. embedding compound with hormone receptor assays. Am J Clin Pathol, 1984. 82(1): p. 89-92.
43. Schwartz, S.A., M.L. Reyzer, and R.M. Caprioli, Direct tissue analysis using matrix-assisted laser desorption/ionization mass spectrometry: practical aspects of sample preparation. J Mass Spectrom, 2003. 38(7): p. 699-708.
44. Weston, L.A. and A.B. Hummon, Comparative LC-MS/MS analysis of optimal cutting temperature (OCT) compound removal for the study of mammalian proteomes. Analyst, 2013. 138(21): p. 6380-4.
45. Vonsattel, J.P., et al., An improved approach to prepare human brains for research. J Neuropathol Exp Neurol, 1995. 54(1): p. 42-56.
46. Adam, M., et al., The effect of liquid nitrogen submersion on cryopreserved human heart valves. Cryobiology, 1990. 27(6): p. 605-14.
47. Bischof, J., K. Christov, and B. Rubinsky, A morphological study of cooling rate response in normal and neoplastic human liver tissue: cryosurgical implications. Cryobiology, 1993. 30(5): p. 482-92.
48. Leidenfrost, J.G., C. Embach, and C.S.E. Wares, A Tract about Some Qualities of Common Water. 1964: Carolyn S.E. Wares.
49. Wu, J.S., G.R. Hogan, and J.D. Morris, Modified methods for preparation of cryostat sections of skeletal muscle. Muscle Nerve, 1985. 8(8): p. 664-6.
50. Crawford, D., et al., New storage procedure for human tumor biopsies prior to estrogen receptor measurement. Cancer Res, 1984. 44(6): p. 2348-51.
51. Mellen, P. and G. Clark, Isopentane frozen sections for intraoperative diagnosis. J Histotechnol, 1991. 14(4): p. 285.
52. Erickson, Q.L., et al., Flash freezing of Mohs micrographic surgery tissue can minimize freeze artifact and speed slide preparation. Dermatol Surg, 2011. 37(4): p. 503-9.
53. McGinley, D.M., Z. Posalaky, and I.P. Posalaky, The use of fresh-frozen tissue in diagnostic transmission electron microscopy. Ultrastruct Pathol, 1984. 6(1): p. 89-98.
54. McLeay, W.R., et al., Epidermal growth factor receptor in breast cancer: storage conditions affecting measurement, and relationship to steroid receptors. Breast Cancer Res Treat, 1992. 22(2): p. 141-51.
55. Mackey, E.A., et al., Quality assurance in analysis of cryogenically stored liver tissue specimens from the NIST National Biomonitoring Specimen Bank (NBSB). Science of the Total Environment, 1999. 226(2-3): p. 165-176.
56. Muschenheim, F., J.L. Furst, and H.A. Bates, Increased incidence of positive tests for estrogen binding in mammary carcinoma specimens transported in liquid nitrogen. Am J Clin Pathol, 1978. 70(5): p. 780-2.
Acknowledgements
We thank Allison Hubel, Ph.D. (University of Minnesota), The Breast Cancer Campaign Tissue Bank, E. David Litwack (FDA), and Joanne Peter Demchock (NCI) for their consultation and insightful suggestions during the development of this document.