Aug 16, 2025
Intra-articular Injection with Strengthening Exercise and Physiotherapy for Knee Osteoarthritis
- Sunjana Saima Anesha1,
- Md. Zahid Hossain1
- 1Jashore University of Science and Technology



Protocol Citation: Sunjana Saima Anesha, Md. Zahid Hossain 2025. Intra-articular Injection with Strengthening Exercise and Physiotherapy for Knee Osteoarthritis. protocols.io https://dx.doi.org/10.17504/protocols.io.261gekd37g47/v1
License: This is an open access protocol distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Protocol status: Working
We use this protocol and it's working
Created: August 15, 2025
Last Modified: August 16, 2025
Protocol Integer ID: 224778
Keywords: Knee Osteoarthritis, Intra-articular Injection, Strengthening Exercises, Conventional Physiotherapy, physiotherapy for knee osteoarthritis, exercises versus conventional physiotherapy, treatment strategies for knee osteoarthritis, knee osteoarthritis, muscle strength in the injection, years with knee osteoarthritis, greater improvements in pain relief, mcmaster universities osteoarthritis index, conventional physiotherapy, physiotherapy, limb strength, pain relief, strengthening exercise, numeric pain rating scale, muscle strength, mg triamcinolone
Abstract
This randomized controlled, single-blind trial will compare the effectiveness of a 40 mg triamcinolone acetonide intra-articular injection combined with strengthening exercises versus conventional physiotherapy in adults aged 40–70 years with knee osteoarthritis. Sixty participants will be randomly assigned to either the injection-plus-exercise group or the physiotherapy-only group, receiving three sessions per week for eight weeks. Pain will be the primary outcome, measured by the Numeric Pain Rating Scale (NPRS), secondary outcomes—physical function, joint range of motion, lower-limb strength, and mobility—will be evaluated using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), goniometer, 30-Second Sit-to-Stand Test, and Timed Up and Go Test.
The study is expected to show greater improvements in pain relief, mobility, range of motion, and muscle strength in the injection-plus-exercise group compared to physiotherapy alone. These findings may support more effective, evidence-based treatment strategies for knee osteoarthritis in clinical practice.

Guidelines
To ensure accurate and standardized execution of the randomized controlled trial (RCT) evaluating intra-articular corticosteroid (CS) injection combined with strengthening exercises and physiotherapy in knee osteoarthritis, the following guidelines must be followed:
Study Oversight:
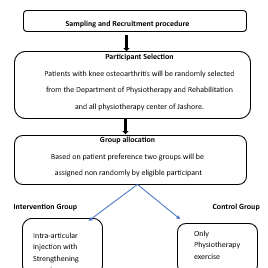
Conduct the single-center RCT at JUST. Randomization will use a computer-generated sequence with allocation concealment via sealed envelopes.
Blinding:
Outcome assessors will be blinded to group allocation.
Training:
Ensure trained professionals perform all interventions.
Orthopedic Surgeon: CS injection administration
Certified Physiotherapist: Supervised strengthening exercises
Assessors: Outcome measurement tools (NPRS, WOMAC, TUG, 30-STS, goniometer)
Participant Screening:
Confirm eligibility based on inclusion criteria: age 40–70, pain, morning stiffness of shorter than 30 minutes or knee crepitus confirmed by a rheumatologist (grades I-III in the Kellgren Lawrence score.
Intervention Delivery:
Control Group: Deliver an 8-week supervised physiotherapy exercise program (3 sessions per week)
Experimental Group: Intra-articular CS injection plus strengthening exercise program starting 7 days post-injection.
Outcome Assessments:
Blinded assessors will measure pain (NPRS), functional mobility (TUG), strength (30-STS), knee ROM (goniometer), and physical function (WOMAC).
Data Management:
Record data on structured forms, anonymize participant information, store in a password-protected database, and conduct regular quality checks to ensure accuracy and completeness.
Materials
Materials
1. Corticosteroid Injection
Preparation: 40 mg Triamcinolone Acetonide, 2% lidocaine
Injection Equipment: 25-gauge needles, 10 ml syringes
2. Strengthening Exercises
Equipment: Resistance bands, ankle weights, floor mats, pillows/bolsters.
Instructional: Printed exercise guides (English/Bengali), home exercise diaries.
Monitoring: Timer, attendance and adherence log sheets.
3. Outcome Assessments
Pain: Numeric Pain Rating Scale (NPRS)
Physical Function & Strength: WOMAC and 30-Second Sit-to-Stand (30-STS) setup (chair, stopwatch), Timed Up and Go (TUG) setup, goniometer for ROM.
4. Data Management
Forms: Data collection sheets for NPRS, WOMAC, TUG, 30-STS, ROM, and adverse events.
Storage: Password-protected computer database, external hard drive/secure cloud storage, locked filing cabinet for physical forms.
5. Safety/Emergency
Supplies: First aid kit, hand sanitizers, surface disinfectants, and emergency contact list.
6. Participant Materials
Informed consent forms and study information sheets (English/Bengali).
Protocol references
1. Bricca, A., Juhl, C. B., Steultjens, M., Wirth, W., & Roos, E. M. (2019). Impact of exercise on articular cartilage in people at risk of, or with established, knee osteoarthritis: a systematic review of randomised controlled trials. British journal of sports medicine, 53(15), 940–947. https://doi.org/10.1136/bjsports-2017-098661
2. Sadeghi, A., Rostami, M., Khanlari, Z.,Zeraatchi, A., Jalili, N., Karimi Moghaddam, A., Karimi Moghaddam, Z., Fallah, R., & Sangtarash, F. (2023). Effectiveness of muscle strengthening exercises on the clinical outcomes of patients with knee osteoarthritis: A randomized four-arm controlled trial. Caspian journal of internal medicine, 14(3), 433–442. https://doi.org/10.22088/cjim.14.3.433
3. Utamawatin, K., Phruetthiphat, O. A., Apinyankul, R., & Chaiamnuay, S. (2023). The efficacy of intra-articular triamcinolone acetonide 10 mg vs. 40 mg in patients with knee osteoarthritis: a non-inferiority, randomized, controlled, double-blind, multicenter study. BMC musculoskeletal disorders, 24(1), 92. https://doi.org/10.1186/s12891-023-06191-6
4. Donec, V., & Kubilius, R. (2019). The effectiveness of Kinesio Taping‱ for pain management in knee osteoarthritis: a randomized, double-blind, controlled clinical trial. Therapeutic advances in musculoskeletal disease, 11, 1759720X19869135. https://doi.org/10.1177/1759720X19869135
5. Jones, C. J., Rikli, R. E., & Beam, W. C.(1999). A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Research quarterly for exercise and sport, 70(2), 113–119. https://doi.org/10.1080/02701367.1999.10608028
6. Henriksen, M., Christensen, R., Klokker, L., Bartholdy, C., Bandak, E., Ellegaard, K., Boesen, M. P., Riis, R. G., Bartels, E. M., & Bliddal, H. (2015). Evaluation of the benefit of corticosteroid injection before exercise therapy in patients with osteoarthritis of the knee: a randomized clinical trial. JAMA internal medicine, 175(6), 923–930. https://doi.org/10.1001/jamainternmed.2015.0461
7. Brumini, C., Furtado, R. N. V., Jones, A., da Silva, R. V. T., & Natour, J. (2025). Effectiveness of prior intra-articular corticosteroid injection in elderly patients with knee osteoarthritis undergoing progressive resistance training: a randomized controlled trial. Advances in rheumatology (London, England), 65(1), 21. https://doi.org/10.1186/s42358-025-00452-9
8. Mohamed, S. H. P., & Alatawi, S. F. (2023). Effectiveness of Kinesio taping and conventional physical therapy in the management of knee osteoarthritis: a randomized clinical trial. Irish journal of medical science, 192(5), 2223–2233. https://doi.org/10.1007/s11845-022-03247-9
9. Lind, V., Svensson, M., & Harringe, M. L. (2021). Reliability and Validity of a Digital Goniometer for Measuring Knee Joint Range of Motion. Measurement in Physical Education and Exercise Science, 26(3), 191–198. https://doi.org/10.1080/1091367X.2021.2004150
10. Alghadir, A., Anwer, S., & Brismée, J. M. (2015). The reliability and minimal detectable change of Timed Up and Go test in individuals with grade 1-3 knee osteoarthritis. BMC musculoskeletal disorders, 16, 174. https://doi.org/10.1186/s12891-015-0637-8
Acknowledgements
We sincerely thank the Department of Physiotherapy & Rehabilitation (PTR) at Jashore University of Science and Technology for partial funding support and for providing the necessary facilities to conduct this trial. We acknowledge the valuable contributions of the Orthopedic Surgeon for administering intra-articular corticosteroid injections, the Physiotherapists for supervising the strengthening exercise program, and all members of the research team for their dedication to implementing this protocol. We also extend our appreciation to the study participants for their time and commitment.