Apr 20, 2026
Version 4
Feasibility assessment of double-blind, crossover, random controlled trial protocol comparing two oxygen-supplemented pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: A pilot study V.4
- Akihiro Ito1,
- Akane Morito2,
- Masahiro Ishizaka1,
- Yukihiro Ogawa2,
- Yuki Kawai2,
- Yuta Hanawa2,
- Naotaka Onodera2,
- Yoshiaki Endo1,
- Isato F ukushi3,
- Kotaro Takeda4,
- Taichi Mochizuki5,
- Yasushi Inoue5,
- Yasuo To6,
- Kazuyuki Chibana7,
- Hideaki Yamasawa8,
- Satoshi Fuke9,
- Sarah Kesler10,
- David Gozal11,
- Yasumasa Okada12,
- Akira Umeda13
- 1Department of Physical Therapy, School of Health Science, International University of Health and Welfare;
- 2Department of Rehabilitation, International University of Health and Welfare Shioya Hospital;
- 3Graduate School of Health Sciences, Aomori University of Health and Welfare;
- 4Faculty of Rehabilitation, School of Health Sciences, Fujita Health University;
- 5Department of Respiratory Diseases Center, International University of Health and Welfare Mita Hospital;
- 6Department of General Medicine, St. Marianna University School of Medicine;
- 7Department of Pulmonary Medicine, Dokkyo Medical University;
- 8Department of Pulmonary Medicine, International University of Health and Welfare Hospital;
- 9Department of Respiratory Diseases Center, KKR Sapporo Medical Center;
- 10Intensive Care Unit, University of Minnesota;
- 11Joan C. Edwards School of Medicine, Marshall University, Huntington, WV, United States of America;
- 12Department of Internal Medicine, Murayama Medical Center;
- 13Department of General Medicine, School of Medicine, IUHW Shioya Hospital, International University of Health and Welfare (IUHW)



Protocol Citation: Akihiro Ito, Akane Morito, Masahiro Ishizaka, Yukihiro Ogawa, Yuki Kawai, Yuta Hanawa, Naotaka Onodera, Yoshiaki Endo, Isato F ukushi, Kotaro Takeda, Taichi Mochizuki, Yasushi Inoue, Yasuo To, Kazuyuki Chibana, Hideaki Yamasawa, Satoshi Fuke, Sarah Kesler, David Gozal, Yasumasa Okada, Akira Umeda 2026. Feasibility assessment of double-blind, crossover, random controlled trial protocol comparing two oxygen-supplemented pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: A pilot study. protocols.io https://dx.doi.org/10.17504/protocols.io.x54v9bdxml3e/v4Version created by Akihiro Ito
License: This is an open access protocol distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Protocol status: Working
We use this protocol and it's working
Created: April 18, 2026
Last Modified: April 20, 2026
Protocol Integer ID: 315287
Keywords: supplemented pulmonary rehabilitation, pulmonary rehabilitation for patient, pulmonary rehabilitation, oxygen supplementations during pr, oxygen supplementation during pr facilitate, copd assessment test score, patients with chronic obstructive pulmonary disease, patients with copd, chronic obstructive pulmonary disease, oxygen supplementation method, oxygen supplementation, copd, flow nasal cannula, pr for patient, physiological benefit, types of oxygen supplementation, respiratory function, muscle strength, rehabilitation
Funders Acknowledgements:
Akihiro Ito
Grant ID: 24K20446
Abstract
_Background_: Pulmonary rehabilitation (PR) for patients with chronic obstructive pulmonary disease (COPD) improves exercise tolerance and COPD assessment test score (CAT). Oxygen supplementation during PR facilitates exercise physiological benefits. This study aimed to assess the feasibility of a trial comparing two oxygen supplementation methods, with the hypothesis that both would be valid and produce distinct outcomes.
_Methods_: This double-blind, crossover, randomized controlled trial compared PR including two types of oxygen supplementation (FiO2 0.3 or 0.5) for patients with COPD (n=6) using a high-flow nasal cannula. Data on the 6MWD, CAT, muscle strength, body composition analysis, respiratory function, and joint range of motion data were collected. Participants underwent one month of regular PR followed by two months of oxygen-supplemented PR, with data collected again after this period. Statistical significance was set at 0.05 with a power of 0.8, and the required sample size was calculated accordingly.
_Results_: The required sample size could not be calculated based on the 6MWD. The improvement in CAT by FiO2 0.3 PR was greater than that by FiO2 0.5 PR. The standardized effect size and the corresponding required sample sizes for the CAT, quadriceps muscle power, lower leg circumference, trunk muscle mass, and leg muscle mass were 0.32/81, 0.66/8, 0.17/114, 0.27/88, and 0.24/56, respectively.
_Conclusions_: Given the small number of participants, the 6MWD and CAT were not appropriate primary endpoints for comparing the effectiveness of the two oxygen supplementations during PR in patients with COPD. However, the quadriceps muscle power was identified as the most suitable primary endpoint among all the investigated parameters.
Image Attribution
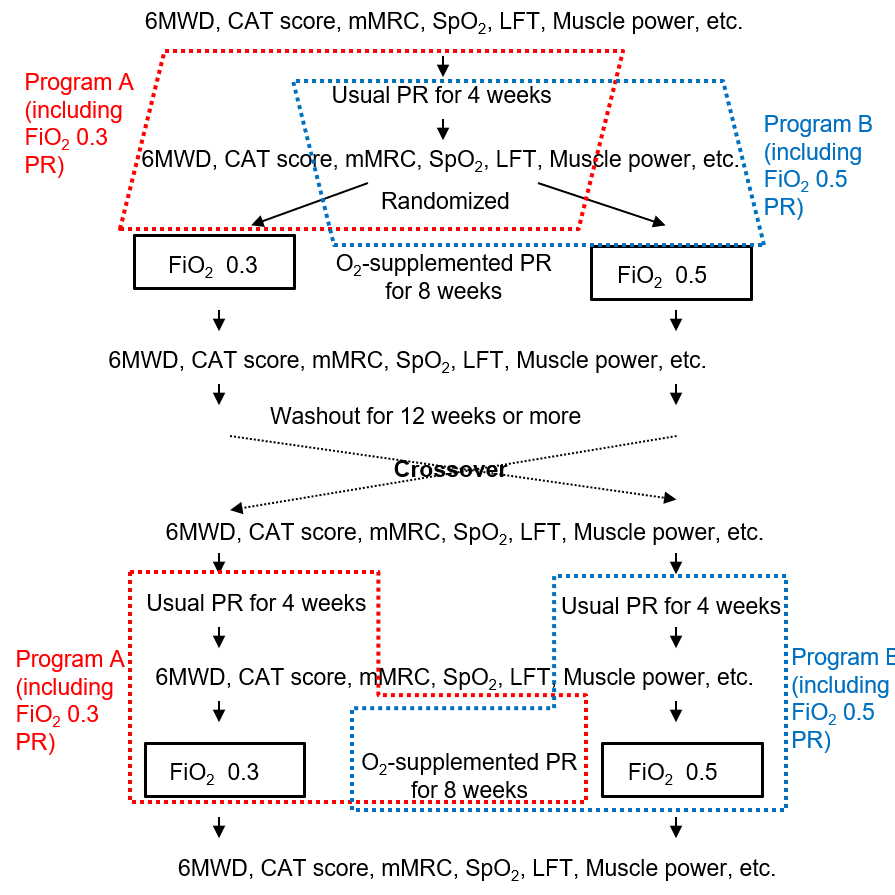
Fig 1. Protocol. Abbreviations: 6MWD, Six-Minute Walk Distance; CAT, COPD Assessment Test; mMRC, Modified Medical Research Council Dyspnea Scale; LFT, Lung function tests; PR, pulmonary rehabilitation.
Guidelines
The treadmill speed was adjusted to target a breathing difficulty level of 4–5 on the revised Borg scale, which is a guideline for aerobic exercise, and the discontinuation criteria were based on the guidelines of the American College of Sports Medicine.
Materials
- Mobie dynamometer (SAKAI med, Japan)
- Tape measure
- Body composition analyser MC-780A-N (TANITA, Japan)
- CHESTAC-8900 respiratory function tester (CHEST, Tokyo, Japan)
- NKV-330 ventilator (Nihon Kohden)
- Transcutaneous Monitor-4 (Radiometer Medical ApS, Denmark)
Safety warnings
Concerns have been raised that both low and high flow rates could lead to issues, such as CO2 accumulation and over-reduction. Additionally, high flow rates may increase discomfort and should be considered.
Ethics statement
This double-blind, crossover, randomized controlled trial was reviewed and approved by the International University of Health and Welfare Ethics Committee according to the Declaration of Helsinki (approval number: 21-B-4). All patients provided written informed consent to participate in the study. This study is registered at the University Hospital Medical Information Network (UMIN) Clinical Trials Registry (registration number: UMIN000047507).
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the top 3 causes of deaths worldwide (cardiovascular diseases, cancer, and COPD),and nearly 90% of these deaths occur in low and middle-income countries [1]. The prevalence of COPD varies widely by region, age, and the availability of
diagnostic spirometry [1]. It accounts for approximately 5% of respiratory-related deaths and is a
leading cause of death in the elderly population [1]. COPD is caused by smoking, air pollution, biomass exposure, occupational dusts, and host factors (including abnormal lung development and lung aging), which is characterized by reduced alveolar ventilation due to alveolar destruction and ventilation/blood flow imbalance [1, 2]. This results in dyspnea, chronic cough, and increased sputum production [3]. Additionally, it causes a decline in physical function, such as exercise tolerance and muscle weakness, and reduces quality of life [4, 5].
Pulmonary rehabilitation (PR) plays an important role in the management of patients with COPD by improving exercise tolerance and quality of life, and reducing dyspnea and fatigue [6-12]. The pulmonary rehabilitation program for stable COPD patients typically comprises supervised exercise training lasting approximately 4 to 12 weeks, generally combining strength training with aerobic exercise [13–15]. Oxygen therapy combined with exercise for patients with COPD has been increasingly evaluated and adopted [16-19]. Evidence is gradually emerging regarding the intervention effects of pulmonary rehabilitation combined with oxygen therapy [20].
Recently, there has been growing interest in the potential benefits of oxygen therapy with a high-flow nasal cannula (HFNC) for COPD. HFNC reduces respiratory muscle load by lowering the arterial partial pressure of carbon dioxide, increasing end-expiratory and end-tidal volumes, and decreasing the respiratory rate, which may improve respiratory patterns [21-23]. Rehabilitation with HFNC has been shown to be superior to conventional rehabilitation using a nasal cannula or Venturi mask in improving the 6-minute walk distance (6MWD) and exercise endurance time in patients with COPD [24, 25]. Additionally, exercise training with HFNC may be superior to exercise training with a regular nasal cannula in patients with chronic respiratory failure receiving long-term oxygen therapy [26].
However, most of these studies have focused on in-situ observations with few interventional studies. Additionally, the optimal setting for HFNC has not been adequately investigated. A meta-analysis of HFNC intervention effects found that while some improvements in quality of life and exercise tolerance were observed, the evidence was insufficient [27]. This lack of consistency was partly due to varying HFNC settings across studies.
Therefore, this study aimed to assess the feasibility of a trial comparing HFNC at two FiO2 levels, with the hypothesis that both methods would be valid and differ from each other. This study may maximize the effects of PR, further improve patients' exercise capacity and quality of life, and reduce dyspnea. Moreover, identifying the optimal HFNC setting could enhance its clinical utility and provide a new standard of care for patients with COPD.
Materials and methods
This double-blind, crossover, randomized controlled trial was reviewed and approved by the International University of Health and Welfare Ethics Committee according to the Declaration of Helsinki (approval number: 21-B-4). All patients provided written informed consent to participate in the study. This study is registered at the University Hospital Medical Information Network (UMIN) Clinical Trials Registry
(registration number: UMIN000047507). The protocol described in this peer-reviewed article is published on protocols.io (dx.doi.org/10.17504/protocols.io.x54v9bdxml3e/v1) and is included for printing purposes as S1 File.
Patients with COPD were recruited from the International University of Health and Welfare (IUHW) Shioya Hospital. The diagnosis of COPD was based on forced spirometry showing the presence of a post-bronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) �3c 0.7. Six participants were consecutively recruited for the pilot study from February 2022 to August 2022. At least nine months per participant were required to record the full data.
Study participants were randomly assigned to one of the two groups using random number tables, with one group starting FiO₂ 0.3 PR including oxygen supplementation PR program (FiO2 0.3 PR) and the other starting FiO₂ 0.5 PR including oxygen supplementation PR program (FiO2 0.5 PR). The protocol developed this time is based on the measurement methods employed in prior research [29, 30]. These assignments were unknown to participants and the physical therapists in charge of PR.
The study protocol is illustrated in Figure 1. The participants underwent regular rehabilitation without oxygen supplementation once a week for four sessions (approximately 1 month). They then underwent eight PR sessions once a week (approximately 2 months) with assigned oxygen supplementation. After the
completion of the intervention, a washout period of > 3 months was established. Following the washout period, PR was performed once a week for 12 sessions (approximately 2 months) with crossover oxygen supplementation. The washout period was set according to prior research in order to account for the time it takes for the learning effects of exercise therapy and the intervention effects of aerobic exercise to dissipate [31-33].
A total of six assessments were conducted: at baseline; after the first course of standard rehabilitation; after the first course of PR; after the washout period; after the second course of standard rehabilitation; and at the end of the second course of PR. Evaluations included 6MWD, COPD assessment test (CAT), modified Medical Research Council (mMRC) dyspnea scale, quadriceps strength at knee extension, lower leg circumference, and body composition. Respiratory function was assessed on four occasions: at baseline, after the first course of PR, after the washout period, and at the end of the second course of PR.
The 6MWD was measured once, following the protocol from previous studies [28, 29]; however, the distance for a walking round trip was set to 15 m in this study. Participants walked at their own pace in comfortable clothing, aiming to cover as much distance as possible in 6 min. Rest breaks were allowed during walking, and the physiotherapist in charge encouraged participants to rest if subjective fatigue, dyspnea, or a significant drop in SpO2 (below 90%) were observed. Participants were instructed to walk slowly if SpO2 fell below 85%, and to stop if necessary. Blood pressure, respiratory rate, heart rate, dyspnea, and lower limb fatigue were measured before and after the measurements using the Borg scale.
CAT and mMRC scores were obtained directly from participants using specialized measurement forms [30, 31]. Lower scores indicate better conditions for both scores.
The knee extensor strength was measured using a Mobie dynamometer (SAKAI med, Japan). The participant was seated with the knee joint flexed at 90°, and a band was attached to the distal leg. Isometric contraction was used to assess bilateral muscle strength [32]. Measurements were taken twice, and the maximum value was used.
The circumference of the lower leg was measured using a tape at the point of maximum circumference. Measurements were taken three times, and the median value was used [33].
Body composition was measured using a body composition analyser MC-780A-N (TANITA, Japan). The participants were assessed in a standing position with their feet bare. The measurement periods were set to be the same. Limb and trunk site-specific total muscle mass, body fat percentage, body fat mass, and lean body mass were measured.
Respiratory function was measured using a CHESTAC-8900 respiratory function tester (CHEST, Tokyo, Japan). Lung capacity and forced vital capacity tests were performed using standardized methods [34, 35]. The reference values for the FEV1 predicted values were derived from the Japanese standards [36].
The range of motion (trunk flexion and extension) was measured using the methods of the Japanese Orthopaedic Association, Japanese Association of Rehabilitation Medicine, and Japanese Society of Foot Surgery. Measurements were taken from the lateral aspect of the trunk, with the posterior sacrum as the base axis and the line connecting the first thoracic spinous process and the fifth lumbar spinous process as the axis of motion. Care was taken to ensure that hip motion was not included.
Pulmonary rehabilitation under O2 supplementation with HFNC
The PR protocol consisted of conditioning, resistance exercise (approximately 20 min), resting on a chair, and walking on a treadmill for 20 min under O2 supplementation with HFNC. PR was conducted for approximately 40 min once a week [43, 44]. Conditioning focused on the relaxation and stretching of the
thoracic and respiratory muscles. Resistance exercises were performed mainly on the lower extremities while monitoring for dyspnea. The treadmill speed was adjusted to target a breathing difficulty level of 4–5 on the revised Borg scale, which is a guideline for aerobic exercise, and the discontinuation criteria were based on the guidelines of the American College of Sports Medicine [45]. Oxygen supplementation was provided using a NKV-330 ventilator (Nihon Kohden), with a flow rate set at 20 L/m unless otherwise indicated.The FiO2 was set at 0.3 or 0.5. HFNC was initiated just prior to the start of conditioning and discontinued after the end of the walking exercise on a treadmill, when the participant was resting in a sitting position [Transcutaneous CO2 and O2 monitoring during walking with a high-flow nasal cannula in patients with chronic obstructive pulmonary disease].
During the rehabilitation intervention, the Transcutaneous Monitor-4 (Radiometer Medical ApS, Denmark) was used to monitor PtcCO2 and PtcO2. Since PtcCO₂ values are typically higher than PaCO2 values, many commercially available instruments have adopted a post-measurement adjustment approach, such as subtracting 4–5 mmHg from the directly measured PtcCO2 values for better estimation of the adult PaCO2. However, we did not adopt such an adjustment; both PtcCO2 and PtcO2 were recorded directly from the tcSensor 84 sensor (Radiometer Medical ApS, Denmark).
This approach was applied consistently across all subject runs [29, 46, 47]. Skin sensors were applied to the forearms of the participants following the manufacturer’s recommendations.
Safety of HFNC settings
Previous studies on respiratory rehabilitation interventions using HFNC have employed flow rates ranging from 20 to 60 L/min, which is inconsistent [27]. Concerns have been raised that both low and high flow rates could lead to issues, such as CO2 accumulation and over-reduction. Additionally, high flow rates may increase discomfort and should be considered [48]. Based on the results of previous studies, PtcCO2 and PtcO2 were monitored during rehabilitation using the Transcutaneous Monitor, with flow rates between 20 and 40 L/min. At lower flow rates (20 L/min), no issues with elevated PtcCO2 were observed. However, at higher flow rates (40 L/min), PtcCO2 dropped significantly during and after exercise therapy, and discomfort was reported (Figure 2). Therefore, the flow rate in this study was set at 20 L/min.
Calculation of the number of subjects needed
Power-based sample size calculation is possible for crossover randomized trials using the methods by Grady et al. [49, 50]. It is important to calculate the necessary sample sizes for feasibility assessments in pilot studies. To determine the required sample size, standardized effect sizes were calculated [51], targeting a significance level of 0.05 and power of 0.8. We assumed that both methods (FiO2 0.3 PR and 0.5 PR) had a direction of good effect and would show differences in effectiveness. Initially, the 6MWD was selected as the primary endpoint; however, as the study progressed, we reconsidered its suitability due to cases where 6MWD showed no improvement after PR. Our aim then shifted to identifying a more
appropriate indicator that demonstrated significant gains post-PR to use in calculating the required sample size. A larger standardized effect size corresponds to a smaller sample size, indicating better feasibility [51]. The change in FiO2 0.5 PR compared to that in FiO2 0.3 PR was defined as the effect size (E), and the standard deviation (S) was calculated from all measurements in the six patients with COPD. The standardized effect size was then calculated as E/S.
Statistical analysis
Data are expressed as mean ± standard deviation unless otherwise indicated. Student’s paired t-test compared between baseline and after walking rehabilitation (two-tailed). Additionally, a sub-analysis was conducted to assess correlations among evaluation indices using Spearman’s rank correlation coefficient. Statistical significance was set at p c 0.05. Commercially available statistical software (BellCurve for Excel; Social Survey Research Information Co., Ltd., Tokyo, Japan) and SPSS version 25 (IBM Corp., Armonk, NY, USA) were used for the statistical analyses.
Protocol references
1. Global Initiative for ChronicObstructive Lung Disease (GOLD). GLOBAL GLOBAL STRATEGY FOR THE DIAGNOSIS, MANAGEMENT, AND PREVENTION OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE:
2026 Report [Internet]. 2023. Available from: https://goldcopd.org/2026-gold-report-and-pocket-guide/
2. Grippi MA, Callen JP. Approach to the Patient with Respiratory Symptoms. In: Fishman’s
Pulmonary Diseases and Disorders, Sixth Edition. New York, NY: McGraw-Hill Education; 2023. p. 394–432.
3. West JB, Luks AM. Obstructive Diseases. In: West’s Pulmonary Pathophysiology, the Essentials, Tenth Edition. Philadelphia, PA: Wolters Kluwer; 2022. p. 69–106.
4. Attaway AH, Welch N, Hatipoğlu U, Zein JG, Dasarathy S. Muscle loss contributes to higher morbidity and mortality in COPD: An analysis of national trends. Respirology. 2020;26(1):62–71.
5. Liu W, Liu Y, Li X. Impact of Exercise Capacity Upon Respiratory Functions, Perception of Dyspnea, and Quality of Life in Patients with Chronic Obstructive Pulmonary Disease. Int J Chron Obstruct Pulmon Dis. 2021;16:1529–34.
6. Rochester CL, Alison JA, Carlin B, Jenkins AR, Cox NS, Bauldoff G, et al. Pulmonary Rehabilitation for Adults with Chronic Respiratory Disease: An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2023;208(4):e7–26.
7. Spruit MA, Singh SJ, Garvey C, ZuWallack R, Nici L, Rochester C, et al. An Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances in Pulmonary Rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–64.
8. Bourbeau J, Bhatt SP. Constructing Modern Pulmonary Rehabilitation: Another Brick from the Wall. Am J Respir Crit Care Med. 2023;207(7):804–5.
9. Holland AE, Cox NS, Houchen-Wolloff L, Rochester CL, Garvey C, ZuWallack R, et al. Defining Modern Pulmonary Rehabilitation. An Official American Thoracic Society Workshop Report. Ann Am Thorac Soc. 2021;18(5):e12–29.
10. Rugbjerg M, Iepsen UW, Jørgensen KJ, Lange P. Effectiveness of pulmonary rehabilitation in COPD with mild symptoms: a systematic review with meta-analyses. Int J Chron Obstruct Pulmon Dis. 2015;10:791–801.
11. Kerti M, Balogh Z, Kelemen K, Varga J. The relationship between exercise capacity and different functional markers in pulmonary rehabilitation for COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:717–24.
12. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary Rehabilitation for Chronic Obstructive Pulmonary Disease. Cochrane Database Syst Rev. 2015;2015(2):CD003793.
13. Higashimoto Y, Ando M, Sano A, Saeki S, Nishikawa Y, Fukuda K, et al. Effect of pulmonary rehabilitation programs including lower limb endurance training on dyspnea in stable COPD: A systematic review and meta-analysis. Respir Investig. 2020;58(5):355–66.
14. Neder JA, Marillier M, Bernard AC, James MD, Milne KM, O’Donnell DE. The Integrative Physiology of Exercise Training in Patients with COPD. COPD. 2019;16(2):182–95.
15. Pancera S, Lopomo NF, Porta R, Sanniti A, Buraschi R, Bianchi LNC. Effects of Combined Endurance and Resistance Eccentric Training on Muscle Function and Functional Performance in Patients With Chronic Obstructive Pulmonary Disease: Randomized Controlled Trial. Arch Phys Med Rehabil. 2023;105(3):470–9.
16. Garrod R, Paul EA, Wedzicha JA. Supplemental oxygen during pulmonary rehabilitation in patients with COPD with exercise hypoxaemia. Thorax. 2000;55(7):539–43.
17. Emtner M, Porszasz J, Burns M, Somfay A, Casaburi R. Benefits of Supplemental Oxygen in Exercise Training in Nonhypoxemic Chronic Obstructive Pulmonary Disease Patients. Am J Respir Crit Care Med. 2003;168(9):1034–42.
18. Nonoyama ML, Brooks D, Guyatt GH, Goldstein RS. Effect of Oxygen on Health Quality of Life in Patients with Chronic Obstructive Pulmonary Disease with Transient Exertional Hypoxemia. Am J Respir Crit Care Med. 2007;176(4):343–9.
19. Moga AM, de Marchie M, Saey D, Spahija J. Mechanisms of non-pharmacologic adjunct therapies used during exercise in COPD. Respir Med. 2012;106(5):614–26.
20. M L Nonoyama 1, D Brooks, Y Lacasse, G H Guyatt, R S Goldstein. Oxygen therapy during exercise training in chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2007;2007(2):CD005372.
21. Pisani L, Vega ML. Use of Nasal High Flow in Stable COPD: Rationale and Physiology. COPD. 2017;14(3):346–50.
22. Bräunlich J, Beyer D, Mai D, Hammerschmidt S, Seyfarth HJ, Wirtz H. Effects of Nasal High Flow on Ventilation in Volunteers, COPD and Idiopathic Pulmonary Fibrosis Patients. Respiration. 2013;85(4):319–25.
23. Bräunlich J, Köhler M, Wirtz H. Nasal highflow improves ventilation in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:1077–85.
24. Vitacca M, Paneroni M, Zampogna E, Visca D, Carlucci A, Cirio S, et al. High-Flow Oxygen Therapy During Exercise Training in Patients With Chronic Obstructive Pulmonary Disease and Chronic Hypoxemia: A Multicenter Randomized Controlled Trial. Phys Ther. 2020;100(8):1249–59.
25. Fang TP, Chen YH, Hsiao HF, Cho HY, Tsai YH, Huang CC, et al. Effect of high flow nasal cannula on peripheral muscle oxygenation and hemodynamic during paddling exercise in patients with chronic obstructive pulmonary disease: a randomized controlled trial. Ann Transl Med. 2020;8(6):280.
26. Chihara Y, Tsuboi T, Sumi K, Sato A. Effectiveness of high-flow nasal cannula on pulmonary rehabilitation in subjects with chronic respiratory failure. Respir Investig. 2022 May;60(5):658–66.
27. Oltra G, Ricciardelli M, Virgilio S, Fernandez Parmo D, Ruiz A, Micaela C, et al. High‐flow nasal cannula during pulmonary rehabilitation for people with chronic obstructive pulmonary disease: A systematic review and meta‐analysis. Physiother Res Int. 2024;29(2):e2088.
28. Global Initiative for Chronic Obstructive Lung Disease (GOLD). GLOBAL STRATEGY FOR PREVENTION, DIAGNOSIS AND MANAGEMENT OF COPD: 2022 Report [Internet]. 2022. Available from: https://goldcopd.org/wp-content/uploads/2021/12/GOLD-REPORT-2022-v1.1-22Nov2021_WMV.pdf
29. Umeda A, Morito A, Ishizaka M, Ito A, Ogawa Y, Kawai Y, et al. Transcutaneous CO2 and O2 monitoring during walking with a high-flow nasal cannula in patients with chronic obstructive pulmonary disease. Respir Investig. 2025;63(5):887-897.
30. Chihara Y, Tsuboi T, Sumi K, Tachibana H, Sato A. Effect of high fraction of inspired oxygen and high flow on exercise tolerance in patients with COPD and IPF: A randomized crossover trial. Respir Investig. 2025;63(3):431-437.
31. Grady DG, Cummings SR, Hulley SB. Alternative clinical trial designs and implementation issues. In: Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB (Eds). Designing Clinical Research, 4th Edition. LIPPINCOTT WILLIAMS & WILKINS, a WOLTERS KLUWER business (2013), p. 151-166. Two Commerce Square, Market Street, Philadelphia, PA, USA.
32. Minoguchi H, Shibuya M, Miyagawa T, Kokubu F, Yamada M, Tanaka H, et al. Cross-over comparison between
respiratory muscle stretch gymnastics and inspiratory muscle training. Intern Med. 2002;41(10):805-12.
33. Konstantinos AV, Helen TD, Peter FK, Savvas PT. Physiological alterations to detraining following prolonged combined strength and aerobic training in cardiac patients. Eur J Cardiovasc Prev Rehabil. 2006;13(3):375-80.
34. Beekman E, Mesters I, Hendriks EJM, Klaassen MPM, Gosselink R, van Schayck OCP, et al. Course length of 30 metres versus 10 metres has a significant influence on six-minute walk distance in patients with COPD: an experimental crossover study. J Physiother. 2013;59(3):169–76.
35. Salzman SH, Agarwala P. Six-Minute Walk Test. Chest. 2019;157(3):603–11.
36. Jones PW, Tabberer M, Chen WH. Creating scenarios of the impact of copd and their relationship to copd assessment test (CATTM) scores. BMC Pulm Med. 2011;11:42.
37. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–6.
38. Katoh M. Test-retest reliability of isometric ankle plantar flexion strength measurement performed by a hand-held dynamometer considering fixation: examination of healthy young participants. J Phys Ther Sci. 2022;34(6):463–6.
39. Kiss CM, Bertschi D, Beerli N, Berres M, Kressig RW, Fischer AM. Calf circumference as a surrogate indicator for detecting low muscle mass in hospitalized geriatric patients. Aging Clin Exp Res. 2024;36(1):25.
40. Miller M, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–38.
41. American Thoracic Society. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1995;152:S77-121.
42. Kubota M, Kobayashi H, Quanjer PH, Omori H, Tatsumi K, Kanazawa M. Reference values for spirometry, including vital capacity, in Japanese adults calculated with the LMS method and compared with previous values. Respir Investig. 2014;52(4):242–50.
43. Hans JB, Stefan K, Katrin R, Hans K, Jan KH, Tibor S, et al. Low intensity, long-term outpatient rehabilitation in COPD: a randomised controlled trial. Respir Res. 2012;13(1):86.
44. Brenda O, Annemarie M, Sara R, Judy MB, Doreen J, Ian B. A comparison of twice- versus once-weekly supervision during pulmonary rehabilitation in chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2007;88(2):167-72.
45. American College of Sports Medicine (ACSM). Exercise Prescription for Individuals with Cardiovascular and Pulmonary Diseases. In: ACSM’S Guidelines for Exercise Testing and Prescription, Eleventh Edition. Philadelphia, PA: Wolters Kluwer; 2022. p. 226–75.
46. Umeda A, Ishizaka M, Tasaki M, Yamane T, Watanabe T, Inoue Y, et al. Evaluation of time courses of agreement between minutely obtained transcutaneous blood gas data and the gold standard arterial data from spontaneously breathing Asian adults, and various subgroup analyses. BMC Pulm Med. 2020;20(1):151.
47. Umeda A, Ishizaka M, Ikeda A, Miyagawa K, Mochida A, Takeda H, et al. Recent Insights into the Measurement of Carbon Dioxide Concentrations for Clinical Practice in Respiratory Medicine. Sensors (Basel). 2021;21(16):5636.
48. Prieur G, Medrinal C, Combret Y, Dupuis Lozeron E, Bonnevie T, Gravier F, et al. Nasal high flow does not improve exercise tolerance in COPD patients recovering from acute exacerbation: A randomized crossover study. Respirology. 2019;24(11):1088–94.
49. Grady DG, Cummings SR, Hulley SB. Alternative clinical trial designs and implementation issues. In: Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB (Eds). Designing Clinical Research, 4th Edition. LIPPINCOTT WILLIAMS & WILKINS, a WOLTERS KLUWER business (2013), p. 151-166. Two Commerce Square, 2001 Market
Street, Philadelphia, PA 19103 USA
50. Browner WS, Newman TB, Hulley SB. Estimating sample size and power: applications and examples. In: Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB (Eds). Designing Clinical Research, 4th Edition. LIPPINCOTT WILLIAMS & WILKINS, a WOLTERS KLUWER business (2013), p. 55-83. Two Commerce Square, 2001 Market Street, Philadelphia, PA 19103 USA
51. Noordzij M, Tripepi G, Dekker FW, Zoccali C, Tanck MW, Jager KJ. Sample size calculations: basic principles and common pitfalls. Nephrol Dial Transplant. 2010;25(5):1388–93.