Aug 16, 2025
Effects of Russian Electrical Stimulation on Knee Osteoarthritis
- Jakia Sultana1,
- Ehsanur Rahman1
- 1Department of Physiotherapy and Rehabilitation, Jashore University of Science and Technology



Protocol Citation: Jakia Sultana, Ehsanur Rahman 2025. Effects of Russian Electrical Stimulation on Knee Osteoarthritis. protocols.io https://dx.doi.org/10.17504/protocols.io.kqdg3wr1ev25/v1
License: This is an open access protocol distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Protocol status: Working
We use this protocol and it's working
Created: June 25, 2025
Last Modified: August 16, 2025
Protocol Integer ID: 220992
Keywords: Knee Osteoarthritis, Quadriceps Strengthening Exercises, Russian Electrical Stimulation, effectiveness of russian electrical stimulation, effects of russian electrical stimulation, russian electrical stimulation, adding russian electrical stimulation, knee osteoarthritis, older adults with knee osteoarthritis, strengthening exercise, mcmaster universities osteoarthritis index, assessing pain, muscle strength, sustained benefit, sustained benefits across gender limitation, minute walk test, pressure pain threshold, enhanced quadriceps, pressure pain threshold via algometer
Abstract
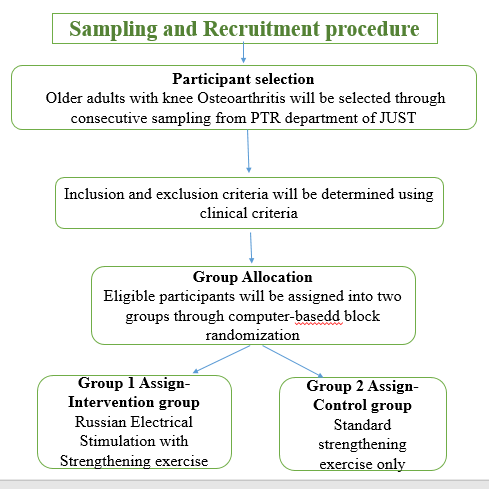
This protocol outlines a randomized controlled trial (RCT) to evaluate the effectiveness of Russian electrical stimulation–enhanced quadriceps strengthening exercise compared with strengthening exercise alone in 70 older adults with knee osteoarthritis, assessing pain, muscle strength, and functional ability over 6 months. The intervention consists of Russian electrical stimulation (50 Hz sinusoidal symmetric pulses, 400 μs pulse duration, 10 ms on/off bursts, 25% duty cycle: 5 s on / 20 s off) combined with a 6-week conventional quadriceps strengthening program. Outcomes will be measured using the VAS scale, pressure pain threshold via algometer, automated portable dynamometer, the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and the 6-Minute Walk Test. This study includes both genders, records baseline OA duration and severity, and evaluates multiple clinically relevant outcomes. It is expected to demonstrate that adding Russian electrical stimulation to strengthening exercise significantly improves pain, muscle strength, and particularly functional outcomes, with sustained benefits across gender limitations.

Guidelines
Guidelines for Protocol Execution
To ensure precise execution of the randomized controlled trial evaluating Russian electrical stimulation–enhanced quadriceps strengthening exercise for older adults with knee osteoarthritis, the following guidelines must be followed:
Study Oversight:
- Conduct the single-center RCT at the Department of Physiotherapy, Jashore University of Science and Technology.
- Randomize participants using block randomization by a computer-generated sequence with allocation concealment via sealed opaque envelopes.
Blinding:
- Outcome assessors measuring pain, muscle strength, and functional ability (VAS, PPT, dynamometer, WOMAC) must be blinded to group allocation.
- Participants will be blinded about group allocation procedure, and therapists cannot be blinded due to the nature of Russian electrical stimulation.
Training:
- Physiotherapists delivering exercises must have certified training in quadriceps strengthening and Russian electrical stimulation.
- Assessors must be trained in VAS scoring, pressure pain threshold measurement, dynamometer use, and WOMAC assessment.
Participant Screening:
- Include older adults aged 60+ years with clinically diagnosed knee osteoarthritis, according to ACR criteria and Kellgren–Lawrence grade.
- Exclude participants with contraindications to electrical stimulation, severe comorbidities, or recent knee surgery.
Intervention Delivery:
- Control Group: Deliver 6-week supervised quadriceps strengthening program (3 sessions/week, 45–50 min each; warm-up, strengthening, non-specific control activities, pain-free positioning, cool-down).
- Experimental Group: Deliver identical strengthening program with additional 10–15 min Russian electrical stimulation per session (50 Hz, 10 ms on/off bursts, 400 μs pulse duration, 25% duty cycle, at maximum patient tolerance).
Outcome Assessments:
- Assess pain (VAS, PPT), quadriceps strength (dynamometer), and functional ability (WOMAC and 6MWT) at baseline, 6 weeks, and follow-up after 12 weeks from post-treatment assessment.
- Assessments conducted by blinded assessors to reduce bias.
Data Management:
- Collect data using structured forms; store anonymized data in a secure, password-protected database.
- Conduct weekly audits to ensure accuracy and completeness.
Materials
Materials
1. Intervention Equipment
- Russian current stimulator (50 Hz, 400 μs, 10 ms bursts, 25% duty cycle)
- Self-adhesive electrodes (5×5 cm) with electrode gel
- Lead wires and a stable power supply
- TheraBands (yellow, red, green, blue) and ankle weights (0.5–2 kg)
- Treatment plinths, chairs, and a timer
2. Outcome Assessments
- Visual Analog Scale (VAS) forms (English/Bengali) and pressure algometer
- Hand-held dynamometer (ActivForce 2TM or equivalent)
- WOMAC questionnaires (English/Bengali)
- 6-Minute Walk Test (6MWT) corridor markers and measuring tape
3. Data Management
- Data collection forms (VAS, PPT, strength, WOMAC, 6MWT)
- Adverse event reporting forms
- Computer with database software, secure external/cloud storage
- Locked filing cabinet for paper records
4. Safety and Emergency
- First aid kit and sharps container
- Hand sanitizer and disinfectants
- Emergency contact list
5. Participant Materials
- Informed consent forms (English/Bengali)
- Patient information sheets (English/Bengali)
Protocol references
- Haider, M. Z.-A.-Q., Bhuiyan, R., Ahmed, S., Zahid-Al-Quadir, A., Choudhury, M. R., Haq, S. A., & Zaman, M. M. (2022). Risk factors of knee osteoarthritis in Bangladeshi adults: a national survey. BMC Musculoskeletal Disorders, 23(1), 333. https://doi.org/10.1186/s12891-022-05253-5
- Kellgren, J., & Lawrence, J. (1963). The epidemiology of chronic rheumatism. Atlas of Standard Radiographs of Arthritis, 2, 22-23. https://doi.org/10.1017/s1120962300016322
- Lespasio, M. J. (2017). Knee osteoarthritis: a primer. The Permanente Journal, 21, 16-183. https://doi.org/10.7812/tpp/16-183
- Paillard, T. N. (2005). Electrical stimulation superimposed onto voluntary muscular contraction. Sports Medicine, 35(11), 951-966. https://doi.org/10.2165/00007256-200535110-00003
- Pelfort, X., Torres-Claramunt, R., Sánchez-Soler, J. F., Hinarejos, P., Leal-Blanquet, J., Valverde, D., Monllau, J. C. (2015). Pressure algometry is a useful tool to quantify pain in the medial part of the knee: an intra- and inter-reliability study in healthy subjects. Orthopaedics & Traumatology: Surgery & Research, 101(5), 559-563. https://doi.org/10.1016/j.otsr.2015.03.016
- Stausholm, M. B., Nielsen, S. M., & Arendt-Nielsen, L. (2023). Pain pressure threshold algometry in knee osteoarthritis: intra- and inter-rater reliability. Physiotherapy Theory and Practice, 39(3), 615-622. https://doi.org/10.1080/09593985.2021.2023929
- Ward, A. R. (2002). Russian electrical stimulation: the early experiments. Physical Therapy, 82(10), 1019-1030. https://doi.org/10.1093/ptj/82.10.1019
- Park, S. H., & Hwangbo, G. (2015). Effects of combined application of progressive resistance training and Russian electrical stimulation on quadriceps femoris muscle strength in elderly women with knee osteoarthritis. Journal of Physical Therapy Science, 27(3), 729-731. https://doi.org/10.1589/jpts.27.729
- Pisters, M., Veenhof, C., & Van Dijk, G. M. (2012). The course of limitations in activities over 5 years in patients with knee and hip osteoarthritis with moderate functional limitations: risk factors for future functional decline. Osteoarthritis and Cartilage, 20(6), 503–510. https://doi.org/10.1016/j.joca.2012.02.002
- Ateef, M. K., Ansari, N. A., & Azam, M. (2016). Test–retest reliability and correlates of 6-minute walk test in patients with primary osteoarthritis of knees. Egyptian Pharmaceutical Journal, 11(4), 192-196. https://doi.org/10.4103/0973-3698.192668
Acknowledgements
We express our sincere gratitude to the Department of Physiotherapy & Rehabilitation (PTR) at Jashore University of Science and Technology, Jashore-7408, Bangladesh, for partial funding support and provision of facilities for this study. We also acknowledge the anticipated contributions of physiotherapists, clinical assessors, and the research team for their expertise in implementing this future protocol.