Aug 19, 2025
Effectiveness of Proprioceptive and Plyometric Training on Joint Stability in Athletes Following ACL Injury
- Mamun Mahmud1,
- Dr. Zahid Hossain2
- 1Department of Physiotherapy and Rehabilitation, Jashore University of Science and Technology, Bangladesh;
- 2Assistant Professor, Department of Physiotherapy and Rehabilitation, Jashore University of Science and Technology, Bangladesh



Protocol Citation: Mamun Mahmud, Dr. Zahid Hossain 2025. Effectiveness of Proprioceptive and Plyometric Training on Joint Stability in Athletes Following ACL Injury. protocols.io https://dx.doi.org/10.17504/protocols.io.81wgbwxkngpk/v1
License: This is an open access protocol distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Protocol status: Working
We use this protocol and it's working
Created: August 19, 2025
Last Modified: August 19, 2025
Protocol Integer ID: 225009
Keywords: ACL injury, proprioceptive training, plyometric training, joint stability, rehabilitation, SEBT, IKDC, WOMAC, ACL-RSI., athletes with unilateral acl reconstruction, plyometric training on joint stability, sport readiness in athlete, improving joint stability, combined effectiveness on joint stability, physiotherapy program, effectiveness of proprioceptive, conventional physiotherapy, sport readiness, receiving conventional physiotherapy, integral components of physiotherapy program, unilateral acl reconstruction, return to sport, anterior cruciate ligament, athletic performance, functional return to sport, knee function, athletes in the intervention group, enhancing neuromuscular control, acl injury, term athletic performance, sport in athlete, following acl injury, greater improvements in joint stability, acl injury background, plyometric training in addition, international knee documentation committee, following acl injury background, postural control, neuromuscular control, earlier return to sport, reduced
Funders Acknowledgements:
Dr. Ehsanur Rahman
Grant ID: Department of Physiotherapy and Rehabilitation, Jashore University of Science and Technology (JUST), Jashore-7408, Bangladesh.
Disclaimer
The content of this thesis is the result of the author’s own research and literature review. Any opinions, conclusions, or recommendations expressed herein are solely those of the author and do not necessarily reflect the views of the affiliated institution, supervisors, or funding bodies. The information presented is intended for academic and educational purposes only. While every effort has been made to ensure the accuracy and reliability of the data and references, the author and institution do not accept any responsibility for errors, omissions, or any consequences arising from the use of this material.
Abstract
Background: Anterior cruciate ligament (ACL) injury is among the most common sports-related injuries and is associated with reduced joint stability, impaired functional performance, and psychological barriers to returning to sport. Although conventional physiotherapy focusing on strengthening and mobility is widely used, recent evidence suggests that proprioceptive and plyometric training may provide additional benefits by enhancing neuromuscular control, balance, and confidence. However, limited randomized controlled trials have comprehensively examined their combined effectiveness on joint stability and return-to-sport readiness in athletes following ACL injury.
Objective: The purpose of this randomized controlled trial is to evaluate the effectiveness of proprioceptive and plyometric training, when combined with conventional physiotherapy, in improving joint stability, reducing pain, enhancing functional outcomes, and promoting psychological readiness for return to sport in athletes following ACL injury.
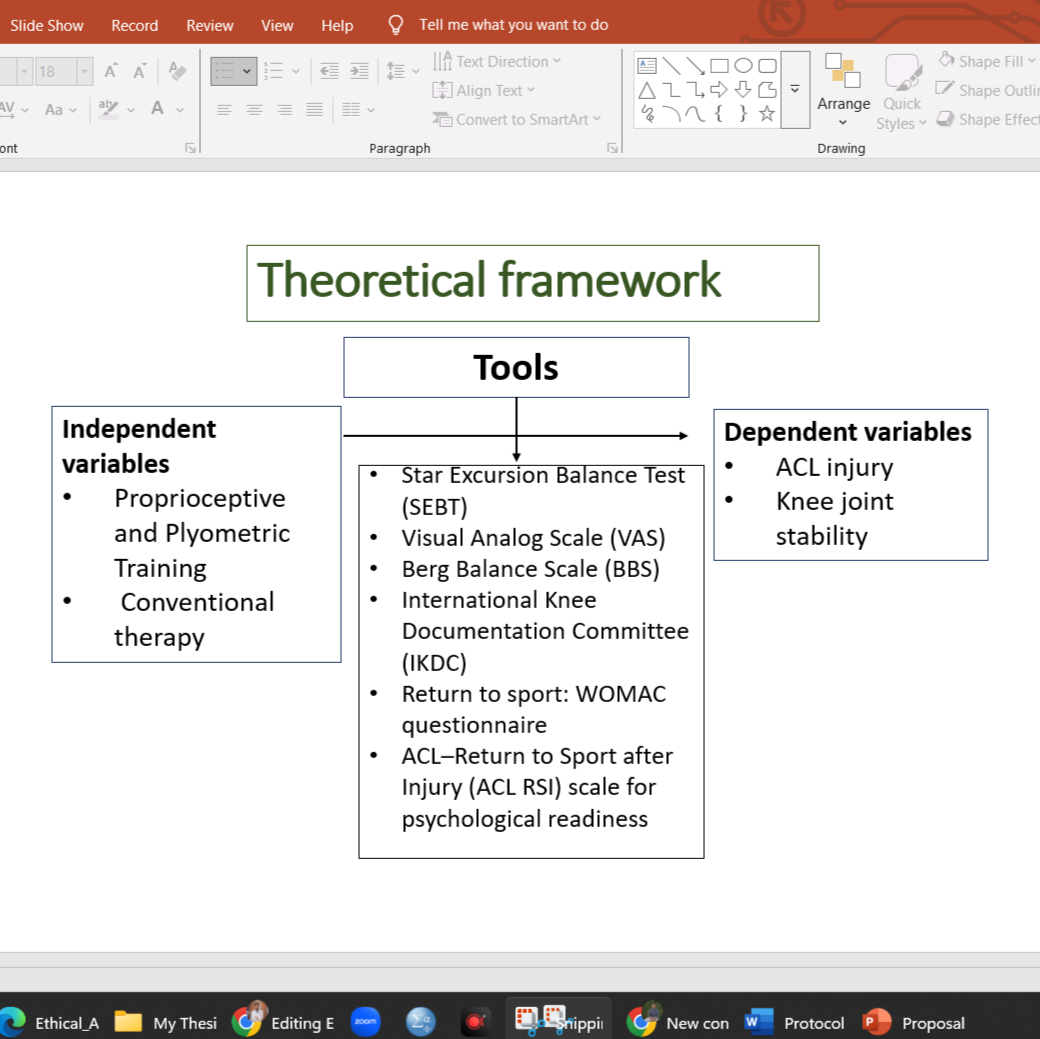
Methods: A total of 62 athletes with unilateral ACL reconstruction will be recruited and randomly assigned into two groups: (i) intervention group (n = 31), receiving proprioceptive and plyometric training in addition to conventional physiotherapy, and (ii) control group (n = 31), receiving conventional physiotherapy alone. The intervention will be carried out over 8 weeks, with supervised sessions two days per week. The primary outcome will be joint stability assessed by the Star Excursion Balance Test (SEBT). Secondary outcomes will include pain measured by the Visual Analog Scale (VAS), postural control assessed by the Berg Balance Scale (BBS), knee function evaluated using the International Knee Documentation Committee (IKDC) subjective score, functional return to sport measured by the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and psychological readiness assessed using the ACL–Return to Sport after Injury (ACL-RSI) scale. Outcomes will be measured at baseline and after the intervention.
Expected Results: It is anticipated that athletes in the intervention group will demonstrate greater improvements in joint stability, pain reduction, balance, knee function, and psychological readiness compared to the control group. Proprioceptive and plyometric training are expected to enhance neuromuscular control and confidence, thereby facilitating safer and earlier return to sport.
Conclusion: This study will provide valuable evidence on the role of proprioceptive and plyometric training in post-ACL rehabilitation. If effective, these approaches may be recommended as integral components of physiotherapy programs to optimize recovery, reduce re-injury risk, and improve long-term athletic performance.
Keywords: ACL injury, proprioceptive training, plyometric training, joint stability, rehabilitation, SEBT, IKDC, WOMAC, ACL-RSI.

Guidelines
Plyometric Training:
1. Standing vertical hops 2sets, 8reps
2. Counter movement jump (CMJ) 2sets, 8reps
3. Depth jumps 2sets, 8reps
4. Multiple two-foot hurdle jumps (hurdle height 0.55m) 2sets, 8reps
5. Two-foot jumps forward and backward 2sets, 8reps
6. Single foot jumps 3sets, 10reps
7. Lateral two-foot jumps 3sets, 10reps
Intervention: Control Group
Conventional therapy:
1. Passive ROM, Patellar mobilization for 5 minutes.
2. Hamstring, quadriceps, calf, hip flexor stretches exercise for 10 minutes and 3 reps, 30 sec, 15 sec rest.
3. Isometric quads 5 minutes and 10 reps, 3sets, 10 sec hold, 15 sec rest.
4. Hamstring curls for 5 minutes and 10 reps, 3sets,15 sec rest.
5. Heel slides for 5 minutes and 10 reps x 3 sets, 2 hold
6. Bridging with double or single leg for 15 minutes and 10 reps x 3 sets, 5 sec hold, 5 sec rest.
7. Closed-chain exercises (mini squats) for 5 minutes and 10 reps x 2 sets, 5 sec rest.
8. Sit-to-stand for 5 minutes and 10 reps x 3 sets, 5 sec rest.
9. Step-ups for 5 minutes and 10 reps x 3 sets, 5 sec rest.
Materials
Musculoskeletal Lab Room - 301, Department of Physiotherapy and Rehabilitation, Jashore University of Science and Technology, Bangladesh.
Tools:
- Star Excursion Balance Test (SEBT)
- Visual Analog Scale (VAS)
- Berg Balance Scale (BBS)
- International Knee Documentation Committee (IKDC)
- WOMAC questionnaire
- ACL–Return to Sport after Injury (ACL-RSI) scale
Safety warnings
- Begin only after medical clearance from your surgeon or physician.
- Always perform exercises under the guidance of a qualified physiotherapist.
- Stop immediately if you feel sharp pain, swelling, dizziness, or instability.
- Do not skip steps — progress must be gradual and patient-specific.
- Exercises should not cause locking, catching, or giving-way of the knee.
- Recovery timelines vary; adapt intensity and volume individually.
- The author and institution are not responsible for misuse or unsupervised application of this protocol.
Ethics statement
This study involving human participants will be conducted in accordance with the Declaration of Helsinki and its later amendments. Ethical approval has been (or will be) obtained from the Institutional Ethics Committee of Jashore University of Science and Technology, Bangladesh.
All participants will provide written informed consent before enrollment. They will be informed about the study objectives, procedures, potential risks, and benefits, and assured of the right to withdraw at any time without any consequence to their medical care. Confidentiality of personal data will be strictly maintained, and all information will be used solely for academic and scientific purposes.
Before start
This rehabilitation protocol is designed for athletes following ACL injury and reconstruction. While the protocol has been applied in practice and shown beneficial outcomes, it must be implemented under the supervision of a qualified physiotherapist or healthcare professional. Individual responses to rehabilitation may vary depending on injury severity, surgical outcomes, and patient-specific factors.
Do not attempt this program without proper medical clearance. The author and affiliated institution do not accept responsibility for any injury, complications, or adverse outcomes resulting from unsupervised or inappropriate application of this protocol.
Intervention details
Intervention: Experimental Group
Proprioception Training: for 30 minutes
1. Single-stance balance exercise performed on: a stable surface, an unstable surface (foam), and an unstable surface (wobble board) with open eyes and closed eyes.
2. Single-stance balance exercise throws the ball in different directions on a stable and unstable surface.
3. Single-stance balance exercise proprioceptive neuromuscular facilitation (PNF) with TheraBand.
4. Single-leg cone pick-up
5. Single-leg balance with ball toss
Plyometric Training: for 30 minutes
1. Standing vertical hops 2sets, 8reps
2. Counter movement jump (CMJ) 2sets, 8reps
Protocol references
10.17504/protocols.io.81wgbwxkngpk/v1
Majewski, M., Susanne, H., & Klaus, S. (2006).
Epidemiology of athletic knee injuries: A 10-year study. The Knee, 13(3),
184–188. https://doi.org/10.1016/j.knee.2006.01.005
Zheng, Q.,Sun, J., Wang, R., Ma, Y., & Chen, P. (2025). Does proprioceptive training
improve joint function and psychological readiness in patients after anterior
cruciate ligament reconstruction? A randomized controlled trial. BMC
Musculoskeletal Disorders, 26(1). https://doi.org/10.1186/s12891-025-08621-z
Başar, B., Başar, G., Aybar, A., Kurtan, A., & Başar, H.
(2020). The effects of partial meniscectomy and meniscal repair on the knee
proprioception and function. Journal of Orthopaedic Surgery, 28(1),
230949901989491. https://doi.org/10.1177/2309499019894915
Moezy, A.,Olyaei, G., Hadian, M., Razi, M., & Faghihzadeh, S. (2008). A comparative
study of whole body vibration training and conventional training on knee
proprioception and postural stability after anterior cruciate ligament
reconstruction. British Journal of Sports Medicine, 42(5), 373–385. https://doi.org/10.1136/bjsm.2007.038554
Barrack, R. L., Skinner, H. B., & Buckley, S. L. (1989).
Proprioception in the anterior cruciate deficient knee. The American Journal of
Sports Medicine, 17(1), 1–6. https://doi.org/10.1177/036354658901700101
Chmielewski, T. L., George, S. Z., Tillman, S. M., Moser, M.
W., Lentz, T. A., Indelicato, P. A., Trumble, T. N., Shuster, J. J., Cicuttini,
F. M., & Leeuwenburgh, C. (2016). Low- versus High-Intensity Plyometric
Exercise during rehabilitation after anterior cruciate ligament reconstruction.
The American Journal of Sports Medicine, 44(3), 609–617. https://doi.org/10.1177/0363546515620583
Hajouj, E., Hadian, M. R., Mir, S. M., Talebian, S., &
Ghazi, S. (2021). Effects of Innovative Aquatic Proprioceptive Training on Knee
Proprioception in Athletes with Anterior Cruciate Ligament Reconstruction: A
Randomized Controlled Trial. PubMed, 9(5), 519–526. https://doi.org/10.22038/abjs.2020.50106.2485
Kazemnejad, A., Asosheh, A., Moezy, A., &
Abasi, A. (2023). Therapy-based expert system on function and postural
stability after anterior cruciate ligament reconstruction: a pilot study. BMC
Musculoskeletal Disorders, 24(1). https://doi.org/10.1186/s12891-023-06735-w
Acknowledgements
Principal investigator/researcher with contact:
Mamun Mahmud
MPT - Sports Medicine (Fellow), Department of Physiotherapy and Rehabilitation, JUST
Email: [email protected] Contact: +8801882481631
Supervisor(s) with contact:
Dr. Zahid Hossain
Assistant Professor, Department of Physiotherapy and Rehabilitation, JUST
Email: [email protected] Contact: +880101670962775
Funding source(s) with contact:
This study will be partially funded by the Department of Physiotherapy and Rehabilitation, JUST