Oct 08, 2025
Community-Academic Partnerships and Healthcare Workforce Development in Underserved Areas: A Scoping Review Protocol
- Khadija Mohd AlSulaimi1,
- Mersiha Kovacevic2,
- Raed Rafeh3,
- Sara Kazim4,
- Wail Bamadhaf5,
- Zeyad Alrais6,
- Aysha Alsharhan7,
- Jukha Shater Al Marzooqi8,
- Nabil Zary2
- 1Latifa Hospital, Dubai Health;
- 2Institute of Learning, Mohammed Bin Rashid University of Medicine and Health Sciences, Dubai Health;
- 3DAI, Dubai Health;
- 4Emergency Medicine Department, Dubai Health;
- 5Graduate Medical Education, Mohammed Bin Rashid University of Medicine and Health Sciences, Dubai Health;
- 6Critical Care Department, Dubai Health;
- 7Hamdan Bin Rashid Cancer Hospital, Dubai Health;
- 8Al Jalila Children’s Specialty Hospital, Dubai Health
- NeuroInk



Protocol Citation: Khadija Mohd AlSulaimi, Mersiha Kovacevic, Raed Rafeh, Sara Kazim, Wail Bamadhaf, Zeyad Alrais, Aysha Alsharhan, Jukha Shater Al Marzooqi, Nabil Zary 2025. Community-Academic Partnerships and Healthcare Workforce Development in Underserved Areas: A Scoping Review Protocol. protocols.io https://dx.doi.org/10.17504/protocols.io.5jyl88w49l2w/v1
License: This is an open access protocol distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Protocol status: Working
We use this protocol and it's working
Created: October 07, 2025
Last Modified: October 08, 2025
Protocol Integer ID: 229204
Keywords: Community partnerships, academic-community collaboration, workforce development, rural health, underserved areas, distributed medical education, social accountability, pipeline programs, recruitment, retention, community engagement, academic partnerships in workforce development, distributed healthcare education, academic partnership, healthcare workforce development, healthcare workforce development in underserved area, healthcare workforce development outcomes in underserved region, academic partnership model, healthcare workforce development outcome, collaborations between academic institution, healthcare education, healthcare professionals in underserved area, partnership, health workforce pipeline stage, models of such partnership, healthcare professional, collaboration, workforce outcome, such partnership, partnership model, fragmented evidence on effective partnership model, academic institution, partnership quality framework, effective partnership model, partnership feature, workforce result, communit
Abstract
Introduction
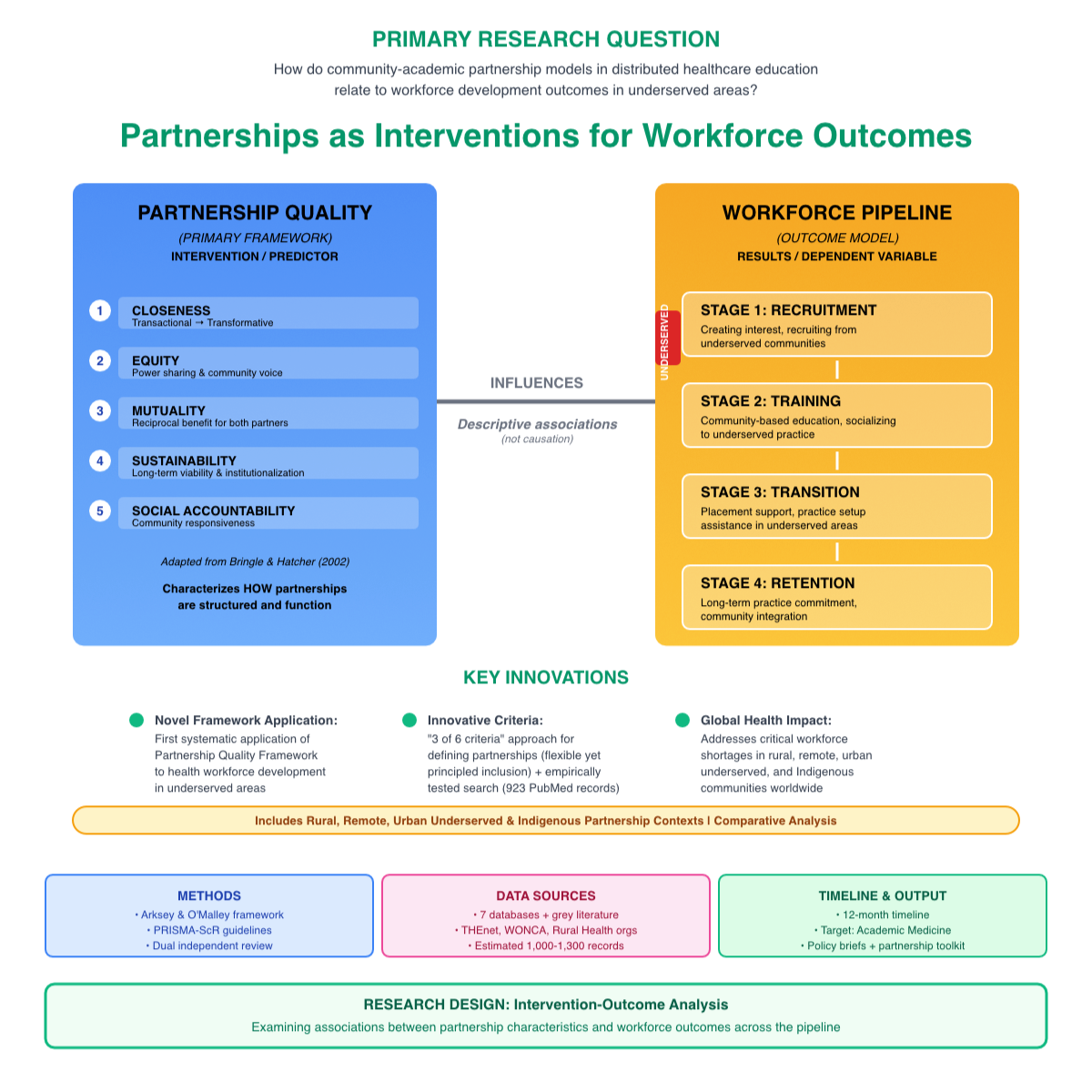
Distributed healthcare education often involves collaborations between academic institutions and community sites to alleviate workforce shortages in underserved regions. These partnerships seek to establish recruitment and training pathways where learners are trained in underserved communities and then practice there. Nonetheless, the models of such partnerships differ greatly in their structure, quality, and success.
Gap Statement
Despite the common use of community-academic partnerships in workforce development, there is still fragmented evidence on effective partnership models, how partnership features relate to workforce results, and methods for maintaining these collaborations. Program leaders often lack guidance grounded in evidence to help them design partnerships that effectively recruit, train, and retain healthcare professionals in underserved areas.
Purpose
To systematically identify community-academic partnership models in distributed healthcare education and analyze how they relate to healthcare workforce development outcomes in underserved regions.
Methods Summary
Following Arksey and O'Malley's framework, enhanced by Levac, and adhering to PRISMA-ScR guidelines, this review will analyze community-academic partnerships in distributed healthcare education from 2015 to 2025. The search will include databases such as PubMed/MEDLINE, Embase, Scopus, CINAHL, Web of Science, ERIC, and relevant grey literature. Two independent reviewers will screen studies using clear operational definitions. Data extraction will be conducted using Bringle & Hatcher's Partnership Quality Framework to describe partnerships. At the same time, workforce outcomes will be categorized according to the WHO's Health Workforce Pipeline stages, including recruitment, training, transition, and retention. The findings will synthesize partnership models, highlight strategies at each stage of the pipeline, and explore the links between partnership features and workforce outcomes.
Image Attribution
Created using Affinity Designer 2 (NZ)
Guidelines
This protocol follows:
- PRISMA Extension for Scoping Reviews (PRISMA-ScR) Checklist
- Arksey and O'Malley Scoping Review Framework (with Levac refinements)
- PRESS (Peer Review of Electronic Search Strategies) guidelines
Materials
Software & Databases
- Covidence systematic review management software
- Reference management software (Mendeley, EndNote, or Zotero)
- Microsoft Word and Excel
- Computer with an internet connection
Database Access Required
- PubMed/MEDLINE
- Embase
- Scopus
- CINAHL
- Web of Science
- ERIC
- Google Scholar
- Rural Health Information Hub
Before start
Prerequisites
- Research team assembled (2+ reviewers, 1 research librarian)
- Covidence license obtained
- Database access confirmed
- Reference management software installed
- Protocol registered on protocols.io
- All team members are trained on scoping review methodology
Expected Duration
12 months from search to manuscript submission
Difficulty Level
Advanced (requires systematic review experience)
IDENTIFY THE RESEARCH QUESTIONS
Define Primary Research Question
How do community-academic partnership models in distributed healthcare education relate to workforce development outcomes in underserved areas?
Define Secondary Research Questions
2.1 What are the characteristics and quality dimensions of community-academic partnerships in distributed healthcare education for underserved areas?
2.2 What workforce development outcomes (recruitment, practice location, retention) are reported in partnership-based programs, and at which pipeline stages do partnerships focus their efforts?
2.3 What partnership characteristics and strategies are associated with successful workforce development outcomes?
2.4 How do partnerships achieve mutual benefit for academic institutions and community partners?
2.5 What factors facilitate or impede partnership sustainability and workforce development success?
Articulate Study Objectives
Primary Objective
To examine community-academic partnership models in distributed healthcare education and their relationship to healthcare workforce development outcomes in underserved areas.
Secondary Objectives
3.1 To characterize partnership models using Partnership Quality Framework dimensions (closeness, equity, mutuality, sustainability, social accountability)
3.2 To describe workforce development outcomes organized by pipeline stages (recruitment, training, transition, retention) and catalogue strategies used at each stage
3.3 To explore associations between partnership quality dimensions and workforce development outcomes
3.4 To examine how partnerships achieve mutual benefit for academic and community partners and factors affecting sustainability
3.5 To identify challenges, barriers, facilitators, and success factors for community-academic partnerships focused on workforce development
IDENTIFY RELEVANT STUDIES
Define Population, Concept, Context (PCC)
Population
Primary: Healthcare learners (medical, nursing, pharmacy, allied health students; residents; fellows) training in community partnership programs
Secondary: Community partners, academic partners, program leaders, and community members involved in partnership governance
Rationale: Workforce development affects learners (career choices, practice location), but partnerships involve multiple stakeholders whose perspectives inform partnership quality and sustainability.
Concept
Included Concepts:
- Community-academic partnerships
- Partnership models and quality
- Collaboration structures
- Workforce development strategies and outcomes
- Recruitment pipelines
- Community-based training
- Retention mechanisms
- Social accountability
- Mutual benefit
- Community engagement
- "Grow your own" programs
Excluded Concepts:
- Partnerships focused solely on research (without education/workforce development)
- International medical graduate pathways (different workforce mechanism)
- Single rotation experiences without ongoing partnership
- Telehealth delivery models without a community partnership element
- Partnerships in well-served urban academic centers (not underserved contexts)
Context
Setting:
Distributed healthcare education programs involving ongoing partnerships between academic institutions and community sites in underserved areas.
Definition of "Underserved Areas":
Communities experiencing healthcare workforce shortages, limited access to healthcare, or health disparities. Includes:
- Rural and remote areas (geographic isolation, low population density)
- Urban underserved areas (poverty, limited access despite population density)
- Indigenous/Aboriginal communities (unique healthcare needs, cultural considerations)
- Medically underserved areas (HRSA designation or equivalent)
Definition of "Partnership":
Ongoing relationship (not single rotation) between academic institution and community site(s) involving shared goals, regular communication, and mutual engagement beyond simple site utilization.
Minimum Criteria for Partnership (must meet at least 3 of 6):
- Duration: Ongoing relationship (≥2 years), not single rotation
- Communication: Regular formal communication (meetings, committees, structured exchanges)
- Shared goals: Explicit shared objectives beyond site provision
- Mutual engagement: Both partners are actively involved (not just a site host)
- Formalization: Some formal agreement (MOU, contract, or documented understanding)
- Workforce intent: Explicit or implicit goal of workforce development for that community
Rationale:
This definition distinguishes genuine partnerships from transactional site arrangements while remaining inclusive of diverse types of partnerships.
Develop Comprehensive Search Strategy
Databases to Search
Primary Databases:
- PubMed/MEDLINE
- Embase
- Scopus
- CINAHL (nursing and allied health)
- Web of Science
- ERIC (education focus)
Grey Literature:
- Rural Health Information Hub
- THEnet (Training for Health Equity Network)
- WONCA Rural Medical Education resources
- Public reports (HRSA, ARHEN)
Date Range
2015-2025 (10-year window)
Rationale: Contemporary partnerships reflecting current models. The emphasis on social accountability in health professions education grew significantly after 2010. Ten-year window balances comprehensiveness with currency.
Language
English (Arabic/Spanish/French if resources permit)
Construct Search String
Search Strategy Development
(("community partnership*"[tiab] OR "academic-community"[tiab] OR
"community collaboration"[tiab] OR "community engagement"[tiab] OR
"community-academic"[tiab] OR "university-community"[tiab])
AND
("workforce development"[tiab] OR "workforce"[tiab] OR "pipeline"[tiab] OR
"practice location"[tiab] OR "grow your own"[tiab] OR
(("recruitment"[tiab] OR "retention"[tiab]) AND ("rural"[tiab] OR "underserved"[tiab])))
AND
("rural health"[tiab] OR "underserved"[tiab] OR "remote health"[tiab] OR
Indigenous[tiab] OR Aboriginal[tiab] OR "medically underserved"[tiab] OR
"social accountability"[tiab])
AND
("medical education"[tiab] OR "nursing education"[tiab] OR
"health professions education"[tiab] OR "distributed education"[tiab] OR
"community-based education"[tiab]))
AND 2015:2024[pdat]
Core search terms
Concept 1 - Partnerships:
- "community partnership*"
- "academic-community"
- "community collaboration"
- "community engagement"
- "community-academic"
- "university-community"
Concept 2 - Workforce Development:
- "workforce development"
- "workforce"
- "pipeline"
- "practice location"
- "grow your own"
- ("recruitment" AND ("rural" OR "underserved"))
- ("retention" AND ("rural" OR "underserved"))
Concept 3 - Underserved Areas:
- "rural health"
- "rural medical education"
- "underserved"
- "medically underserved"
- "remote"
- "Indigenous" OR "Aboriginal"
- "health equity"
- "social accountability"
Concept 4 - Healthcare Education:
- "medical education"
- "nursing education"
- "health professions education"
- "distributed education"
- "community-based education"
MeSH Terms
Apply the following MeSH terms where appropriate:
- Community-Institutional Relations
- Rural Health Services
- Medically Underserved Area
- Health Manpower
- Health Workforce
- Education, Medical
- Education, Nursing
- Cooperative Behavior
- Community-Based Participatory Research
Conduct Grey Literature Search
Grey Literature Quality Threshold:
Must include:
- Clear description of partnership structure
- Some description of workforce strategies or outcomes
- Multi-year or multi-cohort data (not single-year anecdote)
Rural Health Organizations
Search terms: "partnership" AND "workforce" AND "education"
- Rural Health Information Hub (US) - searchable database and policy briefs
- National Rural Health Association (US) - recent publications and policy papers
- Canadian Rural Health Research Society - conference proceedings and reports
- Australian Journal of Rural Health - recent issues
Social Accountability Networks
Search approach: Review documented partnership programs with workforce outcomes
- Training for Health Equity Network (THEnet) - member school reports and case studies
- WONCA Rural Medical Education Guidebook - case examples
- Social Accountability Portal (Towards Unity for Health) - programs database
Policy Reports
- HRSA (Health Resources and Services Administration) - AHEC and rural training grant reports
- Rural Health Research Gateway - research briefs on workforce
- State/Provincial rural health workforce plans with academic partnerships
- Australian Rural Health Education Network (ARHEN) reports
Conference Proceedings
- WONCA Rural Health Conference (2022-2025) - abstract books
- National Rural Health Conference (US) - recent abstracts
- Rural and Remote Health journal - conference supplements
Document Search Process
Create:
- Search log with dates, databases, and search strings used
- Records retrieved per database
- Any modifications to the search strategy
- Rationale for modifications
Export all citations to reference management software (EndNote, Zotero, Mendeley)
STUDY SELECTION
Prepare Screening Environment
- Import all citations into Covidence.
- Remove duplicate records (automatic + manual review)
- Prepare screening forms with inclusion/exclusion criteria
- Train the screening team on operational definitions
Develop Operational Definitions
Operational Definition: "Community Partnership for Workforce Development"
INCLUDE studies that:
- Describe or evaluate the partnership between academic institution and community site(s) in underserved area
- Meet minimum partnership criteria (at least 3 of 6 criteria from Step 4.3)
- Have explicit or implicit workforce development goal OR report workforce outcomes
- Describe partnership structures, processes, quality, or outcomes
- Report workforce outcomes (recruitment, practice location, retention, career choices)
- Examine the factors that influence partnership success or workforce outcomes.
EXCLUDE studies that:
- Describe single rotations without an ongoing partnership relationship
- Focus on urban academic medical centers without an underserved community focus
- International medical graduate pathways (different workforce mechanism)
- Research-only partnerships without an education/workforce development component
- Telehealth/technology solutions without a community partnership element
- Opinion pieces without a program description or empirical data
Test Cases for Screening
INCLUDE Examples:
✓ "University-rural hospital network partnership for medical student training: 10-year retention outcomes"
Rationale: Clear partnership, underserved (rural), workforce outcomes, longitudinal data
✓ "Community engagement in regional medical school campus development: A participatory approach"
Rationale: Partnership (community engagement), distributed education, underserved context
✓ "Pipeline program recruiting Indigenous students for rural nursing practice: Outcomes and lessons learned"
Rationale: Workforce focus (pipeline), underserved (rural, Indigenous), education component
✓ "Building mutual benefit in academic-community partnerships for health professions education"
Rationale: Partnership focus, mutual benefit, health professions education
EXCLUDE Examples:
✗ "International medical graduates filling rural workforce gaps in Australia"
Rationale: Not community partnership; different workforce mechanism
✗ "Telemedicine expanding specialty care access in rural Montana"
Rationale: Technology solution, not partnership; no education component
✗ "Urban hospital elective providing rural exposure for medical students"
Rationale: Single rotation, not ongoing partnership
✗ "Medical student attitudes toward rural practice after brief exposure"
Rationale: Attitude study without partnership description or outcomes
GREY ZONE Examples:
? "Rural preceptorship program for family medicine residents"
INCLUDE if: Ongoing relationship (≥2 years), communication structure, tracks practice locations
EXCLUDE if: Just rotation logistics without partnership elements
? "Community-based participatory research project with medical school"
INCLUDE if: Has education/training component and workforce development goal
EXCLUDE if: Purely research-focused
Define Inclusion/Exclusion Criteria
Inclusion Criteria
- Partnerships between academic institutions and community sites in underserved areas
- Meet minimum partnership criteria (3 of 6 from Step 4.3)
- Healthcare education and/or workforce development focus
- Describe partnership characteristics, structures, processes, or quality
- Report workforce development strategies or outcomes
- Healthcare learners (medical, nursing, pharmacy, allied health; residents; fellows)
- Any research design (quantitative, qualitative, mixed-methods, program evaluation)
- Grey literature with sufficient detail
- Published 2015-2024
- English language (Arabic/Spanish/French if resources permit)
Exclusion Criteria
- Urban academic centers without underserved focus
- Single rotations without ongoing partnership
- International medical graduate programs
- Research-only partnerships
- Telehealth without community partnership
- Opinion pieces without program description
- Published before 2015
- Non-English (except Arabic/Spanish/French)
Conduct Pilot Screening
Expected Result: Kappa ≥0.70, indicating good inter-rater reliability
12.1 Select 50 random titles/abstracts for pilot
12.2 Two reviewers independently screen using operational definitions
12.3 Calculate inter-rater agreement (Cohen's kappa)
12.4 If kappa <0.70:
- Discuss discrepancies
- Refine operational definitions
- Re-pilot with new 50 citations
- Repeat until kappa ≥0.70
12.5 Document all refinements made
Conduct Full Title/Abstract Screening
Expected Result: List of citations for full-text retrieval
13.1 Two independent reviewers screen ALL title/abstracts
13.2 Apply inclusion/exclusion criteria consistently
13.3 Code each citation as:
- Include (proceed to full-text)
- Exclude (document reason)
- Unsure (discuss with team)
13.4 Resolve conflicts:
- Reviewers discuss discrepancies
- If no consensus, the third reviewer decides
- Document decision rationale
13.5 Track progress in Covidence
Retrieve Full Texts
14.1 Retrieve full texts for all included citations
14.2 For unavailable texts:
- Contact corresponding authors
- Check institutional repositories
- Request through interlibrary loan
- Document as "unobtainable" after two attempts
14.3 Organize full texts in a systematic folder structure
Conduct Full-Text Screening
Expected Result: Final list of included studies
15.1 Two independent reviewers screen all full texts
15.2 Apply the same inclusion/exclusion criteria
15.3 Document specific reasons for exclusion:
- No partnership
- No workforce development
- Wrong population
- Wrong context
- Other (specify)
15.4 Resolve conflicts through discussion or a third reviewer
15.5 Maintain exclusion log with reasons
Create PRISMA-ScR Flow Diagram
Document:
- Records identified through database searching
- Records identified through grey literature
- Records after duplicates removed
- Records screened (title/abstract)
- Records excluded (title/abstract) with reasons
- Full texts assessed for eligibility
- Full texts excluded with reasons
- Studies included in review.
Use PRISMA-ScR template available at: https://www.prisma-statement.org/prisma-2020
DATA CHARTING
Develop Data Extraction Form
Expected Result: Validated extraction form with clear instructions
17.1 Create an extraction form based on research questions
17.2 Include six categories (detailed in Step 18)
17.3 Pilot on five deliberately diverse studies:
- Rural medical education partnership (Africa/Asia/ North-South America)
- Indigenous health workforce partnership (Australia/NZ/Canada)
- Nursing in an underserved urban area
- Multi-site regional network
- Grey literature report
17.4 Two reviewers extract from pilot studies independently
17.5 Compare extractions, calculate agreement
17.6 Refine form based on pilot
17.7 Document all changes
Extract Data from Included Studies
Extraction Process:
- Two independent reviewers extract from each study
- Enter data into the standardized extraction form
- Compare extractions regularly
- Resolve discrepancies through discussion
- Third reviewer for unresolved conflicts
Extraction Categories
CATEGORY 1: STUDY & CONTEXT
Study Identification:
- Study ID (Author-Year)
- Country/Region
- Study Design
- Publication Type
- Funding Source
Program Context:
- Healthcare Discipline(s)
- Education Level
- Community Type (Rural/Remote/Urban Underserved/Indigenous)
- Population Served
- Number of Community Sites
- Program Scale (learners/year)
- Years of Partnership Operation
- Program Maturity
CATEGORY 2: PARTNERSHIP CHARACTERISTICS
Partnership Structure:
- Partners Involved
- Governance Model
- Formalization (MOU, contract, informal)
CATEGORY 3: WORKFORCE DEVELOPMENT STRATEGIES
Pipeline Stage Focus:
For each stage, indicate: ☐ Not addressed / ☐ Minimal / ☐ Moderate / ☐ Major
Recruitment Stage:
- Focus level: [checkbox]
- Brief description: [open text]
Training Stage:
- Focus level: [checkbox]
- Brief description: [open text]
Transition Stage:
- Focus level: [checkbox]
- Brief description: [open text]
Retention Stage:
- Focus level: [checkbox]
- Brief description: [open text]
Comprehensive Pipeline:
- Does it address all four stages? (Yes - all 4 / Partial - 2-3 / Limited - 1 / None)
CATEGORY 4: WORKFORCE OUTCOMES
Study Design:
- Outcome measurement rigor: (Descriptive / Retrospective / Prospective / Quasi-experimental / RCT)
- Comparison group: (No / Yes - describe)
- Follow-up period: [years]
Recruitment Outcomes:
- % students FROM underserved communities
- Diversity metrics
- Student interest in underserved practice
Practice Location Outcomes:
- % practicing in underserved areas
- % in training community specifically
- % in target specialty
- Follow-up time period
Retention Outcomes:
- % still practicing at: 1yr / 3yr / 5yr / 10yr+
- Reasons for staying
- Reasons for leaving
- Comparison data
Other Metrics:
- Specialty choices
- Community health impact
- Workforce shortage mitigation
CATEGORY 5: FACILITATORS, BARRIERS, SUCCESS FACTORS
Facilitators:
- Partnership factors
- Institutional factors
- Community factors
- Policy/funding factors
- Individual factors
Barriers:
- Partnership challenges
- Resource limitations
- Geographic/logistic challenges
- Policy barriers
- Recruitment/retention challenges
Critical Success Factors:
- Authors' identified essentials
- Recommendations
Lessons Learned:
- Key takeaways
- Surprises
- Advice for new partnerships
CATEGORY 6: MUTUAL BENEFIT & SUSTAINABILITY
Academic Benefits:
- Training capacity expansion (Y/N - describe)
- Diverse learning experiences (Y/N)
- Research opportunities (Y/N)
- Community goodwill (Y/N)
- Mission fulfillment (Y/N)
- Other
Community Benefits:
- Workforce recruited/retained (Y/N)
- Enhanced services (Y/N)
- Economic impact (Y/N)
- Capacity building (Y/N)
- Community pride (Y/N)
- Health outcomes (Y/N)
- Other
Balance:
- Primarily academic / Primarily community / Balanced mutual / Unclear
Community Health Impact:
- Access metrics
- Health outcomes
- Health equity outcomes
Sustainability Indicators:
- Partnership active at publication? (Y/N)
- Plans for continuation? (Y/N)
- Threats identified?
- Strategies employed?
Conduct Quality Checks
Expected Result: Consistent, high-quality data extraction
19.1 Weekly team meetings during extraction
19.2 Compare sample extractions regularly
19.3 Maintain decision log for:
- Unclear studies
- Edge cases
- Framework application questions
19.4 Resolve discrepancies promptly
19.5 Calculate inter-rater reliability on subsample
COLLATE, SUMMARIZE, AND REPORT
Prepare Data for Synthesis
Export all extracted data from Covidence
Create synthesis database (Excel/SPSS)
Code and organize data by:
- Partnership quality dimensions
- Pipeline stages
- Context types
- Outcome categories
Check for data entry errors
Create summary tables
Conduct Descriptive Analysis (Part 1: Landscape)
Quantitative Description:
- Number of studies by: country, discipline, education level, community type, publication type
- Partnership duration (range, median, mean)
- Program scale (learners/year)
- Number of partner sites
- Publications per year (2015-2024 trend)
Visual Representations:
- World map: Geographic distribution
- Bar charts: Discipline, community type distributions
- Timeline: Publications per year
- Box plot: Partnership duration
Qualitative Description:
- Overview of partnership contexts
- Overview of study designs
- Overview of outcome measurement approaches
Expected Outputs:
- Descriptive statistics tables
- Summary figures and charts
- Narrative description of the publication landscape
Characterize Partnerships (Part 2)
Analysis by Each Quality Dimension:
CLOSENESS:
- Frequency distribution (Transactional/Cooperative/Collaborative/Transformative)
- Contextual patterns (rural vs. urban vs. Indigenous)
- Evolution patterns
- Examples from literature
EQUITY:
- Distribution (Low/Medium/High)
- Power sharing patterns
- Resource flow patterns
- Community voice in governance
MUTUALITY:
- % reporting mutual benefits
- Common academic benefits
- Common community benefits
- Designed for mutuality
SUSTAINABILITY:
- Duration distribution
- Funding models
- Champion-dependent vs. institutionalized
- Partnerships that ended - why?
SOCIAL ACCOUNTABILITY:
- % addressing community priorities
- Community governance involvement
- Local workforce focus
- Health equity emphasis
Analyze Workforce Strategies (Part 3)
By Pipeline Stage:
RECRUITMENT:
- % of partnerships focusing on recruitment
- Strategy inventory from extractions
- Categorize strategies
- Innovative approaches
- Context-specific patterns
TRAINING:
- % focusing on training
- Strategy inventory
- Training intensity and duration
- Categorization
TRANSITION:
- % focusing on transition (expect least common)
- Strategy inventory
- Categorization
RETENTION:
- % focusing on retention
- Strategy inventory
- Categorization
Comprehensive Pipeline:
- % addressing all 4 stages vs. subset
- Do comprehensive approaches show better outcomes?
Gap Identification:
- Under-addressed stages
- Under-utilized strategies
Examine Partnership-Outcome Associations (Part 4)
For Each Partnership Dimension:
CLOSENESS:
- Extract retention rates by closeness level
- Compare: Do transformative partnerships report higher retention than transactional?
- Note: differences in follow-up timing, measurement, contexts
EQUITY:
- Extract % students from target communities by equity level
- Hypothesis: High-equity partnerships recruit more local students
- Note: confounding factors
MUTUALITY:
- Extract partnership longevity by mutuality
- Hypothesis: Mutual benefit partnerships sustain longer
- Note: reverse causation possible
SUSTAINABILITY:
- Extract consistency of outcomes over time
- Hypothesis: Institutionalized partnerships show stable outcomes
- Note: requires longitudinal data
SOCIAL ACCOUNTABILITY:
- Extract retention in specific training communities
- Hypothesis: High SA → better retention in that community
- Note: definition variations
Cross-Dimensional Patterns:
- Do certain combinations predict outcomes?
- Are some dimensions more important?
- Context differences?
Conduct Contextual Analysis
Compare across:
- Rural/Remote partnerships
- Urban Underserved partnerships
- Indigenous/Aboriginal partnerships
For Each Context:
- Partnership quality profile
- Common workforce strategies
- Typical outcomes
- Unique challenges
- Success factors
Cross-Context Synthesis:
- What's universal?
- What's context-specific?
- Generalizability considerations
Expected Outputs:
- Comparison tables
- Context-specific recommendations
- Universal principles identified
Synthesize Success Factors
Facilitators:
- Most common across partnerships
- Context-specific facilitators
- Critical success factors
- Enablers of mutual benefit
- Enablers of sustainability
Barriers:
- Most common barriers
- Context-specific barriers
- How partnerships overcame them
Best Practices:
- Synthesis of recommendations
- Lessons learned
- Do's and don'ts
Expected Outputs:
- Best practices summary
- Lessons learned synthesis
- Practical recommendations
Identify Research Gaps
Partnership Research Gaps:
- Understudied partnership models
- Understudied contexts
- Understudied disciplines
- Geographic gaps
Workforce Outcome Gaps:
- Understudied pipeline stages
- Understudied outcomes
- Measurement gaps
Methodological Gaps:
- Lack of comparison groups
- Lack of longitudinal studies
- Lack of cost-effectiveness analyses
- Need for theory-driven research
Expected Outputs:
- Research gap summary
- Priority research questions
- Methodological recommendations
Draft Manuscript
Structure:
Introduction
- Background on workforce shortages
- Community-academic partnerships as a solution
- Gap statement
- Objectives
Methods
- Scoping review methodology
- Search strategy
- Selection process
- Data extraction
- Synthesis approach
Results
- Part 1: Landscape (descriptive)
- Part 2: Partnership characterization
- Part 3: Workforce strategies
- Part 4: Partnership-outcome associations
- Part 5: Contextual analysis
- Part 6: Success factors
Discussion
- Summary of key findings
- Interpretation
- Partnership quality and outcomes
- Context considerations
- Research gaps
- Limitations
- Implications for policy and practice
Conclusion
- Key messages
- Recommendations
Include:
- PRISMA-ScR checklist
- All tables and figures
- Supplementary materials
Internal Review and Revision
29.1 Team reviews draft manuscript
29.2 Incorporate feedback
29.3 Verify all data and citations
29.4 Check consistency
29.5 Proofread
29.6 Finalize figures and tables
Submit to Target Journal
Target Journals (Prioritized):
- JMIR Medical Education (IF:12)
- Academic Medicine (IF: 7.7)
- Medical Education (IF: 5.3)
- Rural and Remote Health (IF: 2.1)
- Teaching and Learning in Medicine (IF: 3.2)
- BMC Medical Education (IF: 2.7)
Submission Package:
- Cover letter
- Manuscript
- PRISMA-ScR checklist
- Figures and tables
- Supplementary materials
- Conflict of interest declarations
- Copyright transfer agreements
KNOWLEDGE TRANSLATION OUTPUTS
Develop Policy Brief
Title: "Designing Effective Community-Academic Partnerships for Healthcare Workforce Development: Evidence-Based Guidance"
Audience: Health workforce planners, policymakers, academic leaders, community partners
Content:
- Partnership quality dimensions that matter
- Strategies associated with success
- Common pitfalls
- Context-specific considerations
- Actionable recommendations
Format: 3-4 page brief
Distribution: Government health departments, professional associations.
Create Partnership Self-Assessment Tool
Title: "Assessing Your Community-Academic Partnership: A Quality Framework Tool"
Format: Interactive PDF or web-based
Content:
- Questions assessing five quality dimensions
- Scoring guide
- Interpretation
- Recommendations for improvement
Audience: Partnership leaders
Distribution: Open access via institutional repository, THEnet, WONCA
Develop Partnership Development Toolkit
Title: "Building Win-Win Community-Academic Partnerships: A Practical Toolkit"
Format: Comprehensive guide (15-20 pages)
Content:
- Partnership development stages
- Strategies for mutual benefit
- Governance models with examples
- Sample MOUs
- Evaluation frameworks
- Case examples
- Troubleshooting guide
Audience: Academic and community partners
TIMELINE
Total Duration: 12 months
Month 1:
- Protocol finalization and registration
- Search strategy validation
- Database searches
- Citation management setup
Months 2-3:
- Complete searches
- Grey literature searches
- Deduplication
- Pilot screening
- Begin title/abstract screening
Months 4-5:
- Complete title/abstract screening
- Full-text retrieval
- Full-text screening
Months 6-7:
- Pilot data extraction
- Refine the extraction form
- Begin full data extraction
- Quality checks
Month 8:
- Complete data extraction
- Begin synthesis Part 1-2
Month 9:
- Complete synthesis Part 2-4
- Optional: Stakeholder consultation
Month 10:
- Complete synthesis Part 5-7
- Begin manuscript drafting
- Create visuals
Month 11:
- Complete manuscript draft
- Internal review
- Begin knowledge translation products
Month 12:
- Final revisions
- Submit to a journal
- Submit conference abstracts
- Finalize knowledge translation products
Protocol references
Arksey H, O'Malley L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology. 2005;8(1):19-32.
Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implementation Sci. 2010;5(1):69.
Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467-473.
Bringle RG, Hatcher JA. Campus-community partnerships: The terms of engagement. Journal of Social Issues. 2002;58(3):503-516.
World Health Organization. Global strategy on human resources for health: Workforce 2030. Geneva: WHO; 2016.
Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376(9756):1923-1958.
Boelen C, Heck JE. Defining and measuring the social accountability of medical schools. Geneva: WHO; 1995.
Strasser R, Neusy AJ. Context counts: training health workers in and for rural and remote areas. Bull World Health Organ. 2010;88(10):777-782.
Rabinowitz HK, Diamond JJ, Markham FW, Wortman JR. Medical school programs to increase the rural physician supply: a systematic review and projected impact of widespread replication. Acad Med. 2008;83(3):235-243.
Worley P, Murray R. Social accountability in medical education - an Australian rural and remote perspective. Med Teach. 2011;33(8):654-658.
Rourke J. Social Accountability: A Framework for Medical Schools to Improve the Health of the Populations They Serve. Academic Medicine. 2018;93(8):1120-1124
Acknowledgements
We acknowledge CORE/IoL for assistance with search strategy development and validation. We thank the community partners and academic leaders who will contribute to stakeholder consultation.