Apr 16, 2026
Cardiovascular Health and Lifestyle in Aragón Adolescents (CHIARA): protocol for a longitudinal cohort study integrating cardiovascular, behavioural and psychosocial assessment
- Iris Iglesia Altaba1,2,
- Gerardo Rodríguez-Martínez1,3,4,
- Cristina Guillén-Sebastián1,5,
- Carlos Nagore-González1,5,4,
- María Isabel Iguácel Azorín6,7,
- Miguel Máximo Seral-Cortés6,7,
- María Luisa Miguel-Berges6,7,
- Guiomar Masip6,7,
- Isabel Bendicto6,7,
- Natalia Giménez-Legarre6,7,
- Sheila García Enguita8
- 1Spanish network in maternal, neonatal, child and developmental health research (RICORS-SAMID), Instituto de Salud Carlos III, 28040 Madrid, Spain;
- 2Growth, Exercise, Nutrition and Development (GENUD) Research Group, Universidad de Zaragoza, Instituto Agroalimentario de Aragón (IA2), Instituto de Investigación Sanitaria Aragón (IISAragón), Zaragoza, España.;
- 3Growth, Exercise, Nutrition and Development (GENUD) Research Group, Universidad de Zaragoza, Instituto Agroalimentario de Aragón (IA2), Instituto de Investigación Sanitaria Aragón (IISAragón), Zaragoza, España;
- 4Hospital Clínico Universitario Lozano Blesa, Zaragoza, España;
- 5Instituto de Investigación Sanitaria Aragón (IISAragón), Zaragoza, España;
- 6Growth, Exercise, Nutrition and Development (GENUD), Research Group, Instituto Agroalimentario de Aragón (IA2), Instituto de Investigación Sanitaria Aragón (IIS Aragón) Universidad de Zaragoza, Zaragoza, Spain;
- 7Centro de Investigación Biomédica en Red de Fisiopatología de la Obesidad y la Nutrición (CIBERObn), Instituto de Salud Carlos III, Madrid, Spain;
- 8Instituto de Investigación Sanitaria Aragón (IIS Aragón), Zaragoza, Spain



Protocol Citation: Iris Iglesia Altaba, Gerardo Rodríguez-Martínez, Cristina Guillén-Sebastián, Carlos Nagore-González, María Isabel Iguácel Azorín, Miguel Máximo Seral-Cortés, María Luisa Miguel-Berges, Guiomar Masip, Isabel Bendicto, Natalia Giménez-Legarre, Sheila García Enguita 2026. Cardiovascular Health and Lifestyle in Aragón Adolescents (CHIARA): protocol for a longitudinal cohort study integrating cardiovascular, behavioural and psychosocial assessment. protocols.io https://dx.doi.org/10.17504/protocols.io.14egn5odzg5d/v1
License: This is an open access protocol distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Protocol status: Working
We use this protocol and it's working
Created: April 14, 2026
Last Modified: April 16, 2026
Protocol Integer ID: 315003
Keywords: CARDIOVASCULAR, PROGRAMMING, METABOLIC, COHORT, ADOLESCENCE, lifestyle in aragón adolescent, aragón adolescent, cardiovascular health profile, cardiovascular health across the life course, cardiovascular health, characterization of cardiovascular health profile, studying cardiovascular health, term implications for cardiometabolic health, cardiovascular risk, cardiometabolic health, longitudinal cohort study, late adolescence, characterized longitudinal cohort, adolescent population, adolescent, longitudinal cohort, up of the calina birth cohort, calina birth cohort, emotional health dimension, psychosocial health, early childhood, aragón, body composition, chiara study, blood pressure, years of age, lifestyle behaviour, clinical measurement
Funders Acknowledgements:
Proyecto de I+D+I en salud, Acción Estratégica en Salud 2021-2023 (Instituto de Salud Carlos III)
Grant ID: PI23/01771
Abstract
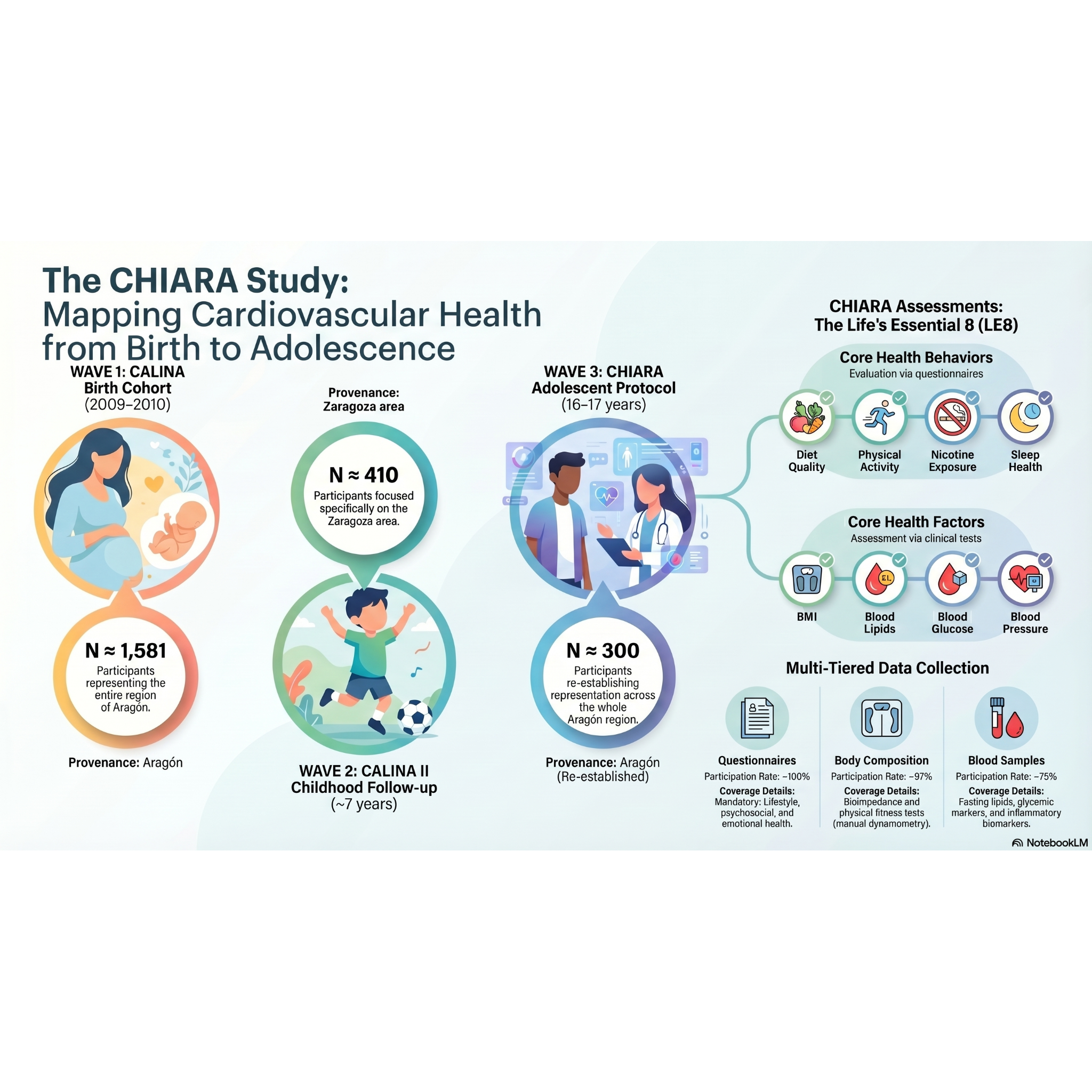
Background: Cardiovascular risk originates early in life and is shaped by a complex interplay of biological, behavioural and psychosocial factors. Late adolescence represents a critical developmental window during which these determinants may have long-term implications for cardiometabolic health. Despite increasing recognition of these early-life influences, there is still a lack of integrative and standardized approaches combining clinical, lifestyle and emotional health dimensions within well-characterized longitudinal cohorts. Methods: The CHIARA study is a follow-up of the CALINA birth cohort, established in Aragón, Spain, in 2009–2010. Participants were previously assessed during early childhood, including a detailed evaluation at approximately 7 years of age. The current wave focuses on adolescents aged 16–17 years and includes a comprehensive assessment integrating questionnaire-based data, clinical measurements and biological sampling. Completion of the questionnaire package was the only mandatory requirement for participation, allowing broad inclusion across the region. Self-reported weight and height were collected in all participants. Optional in-person assessments included body composition measured by bioelectrical impedance (Tanita MC-580), blood pressure and blood sampling. Lifestyle behaviours were assessed using validated instruments, and emotional and psychosocial health were evaluated using standardized questionnaires. The primary outcome is cardiovascular health assessed through the Life’s Essential 8 score. Expected results: This protocol will enable the characterization of cardiovascular health profiles in late adolescence and the identification of associations with lifestyle behaviours, psychosocial factors and early-life determinants. Conclusions: This protocol provides a robust and scalable framework for studying cardiovascular health across the life course and may contribute to the development of early preventive strategies in adolescent populations.
Materials
- Food frequency questionnaire (IDIBAPS)
- International Physical Activity Questionnaire for Adolescents (IPAQ-A)
- Pittsburgh Sleep Quality Index (PSQI)
- I.Family Teen Questionnaire
- Strengths and Difficulties Questionnaire (SDQ)
- Perceived Stress Scale (PSS-10)
- Bergen Social Media Addiction Scale
- Portable stadiometer SECA 213
- Tanita MC-580 (bioelectrical impedance)
- HOLOGIC Horizon DXA scan
- Ergonomic circumference measuring tape SECA201
- Hand grip Takei 5001 Grip-A
- Longitudinal jump test
OBJECTIVES
The main objective of the CHIARA study is to characterize cardiovascular health in late adolescence using the Life’s Essential 8 framework.
Secondary objectives include:
(1) to examine the association between lifestyle behaviours, psychosocial factors and cardiovascular health;
(2) to investigate the role of early-life determinants from the CALINA cohort in shaping adolescent cardiovascular health and what is the influence of socioeconomic determinants;
(3) to identify behavioural and psychosocial profiles associated with cardiovascular risk;
(4) to explore simplified approaches for early cardiovascular risk screening in adolescents.
STUDY DESIGN AND POPULATION
The CHIARA study is a longitudinal follow-up of the CALINA cohort, a population-based birth cohort established in Aragón, Spain (2009–2010) and initially funded by the Instituto de Salud Carlos III (project PI08/0559).
Participants were followed during early childhood, with a subsequent detailed assessment at approximately 7 years of age (project PI13/00105), including evaluation of growth, body composition and lifestyle factors.
The current wave includes approximately 300 adolescents aged 16–17 years from across Aragón, re-establishing regional representation. This design combines longitudinal data from a well-characterized cohort with updated assessments inlate adolescence.
The study is conducted by a multidisciplinary team involving paediatricians, neonatologists, physicians, psychologists, nurses and dietitians-nutritionists, allowing a comprehensive assessment integrating clinical, behavioural and psychosocial domains. From them, those participating in the measurements were appropriately trained.
PARTICIPATION FRAMEWORK
Completion of the questionnaire package was the only mandatory requirement for participation. Its ompletion was performed in an online platform. These approaches were adopted to maximize feasibility and participation in a geographically dispersed population across Aragón, minimizing the burden associated with in-person assessments.
Self-reported weight and height were collected through the questionnaire in all participants, ensuring a minimum common dataset across the cohort. In-person assessments were optional and included body composition, blood pressure, physical fitness and blood sampling.
MEASUREMENTS
Lifestyle and psychosocial assessment
Dietary intake is assessed using the food frequency questionnaire of 151 items developed by IDIBAPS (Instituto de Investigaciones Biomédicas August Pi i Sunyer (IDIBAPS). Physical activity is measured using the International Physical Activity Questionnaire for Adolescents (International Physical Activity Questionnaire for adolescents, IPAQ-A). The Pittsburgh Sleep Quality Index (PSQI) was used to evaluate the sleep quality. Psychosocial and behavioural factors were assessed using a combination of standardized instruments and specific questionnaire items derived from the I.Family Teen Questionnaire (age ≥12 years). Emotional and behavioural difficulties were evaluated using the Strengths and Difficulties Questionnaire (SDQ), while perceived stress was assessed with the Perceived Stress Scale (PSS-10). Problematic social media use was evaluated using the Bergen Social Media Addiction Scale.
In addition, the questionnaire included items addressing subjective well-being and quality of life in relation to oneself, family and peers, as well as body image perception and satisfaction, and aspects of impulsivity and behavioural regulation. Social media use patterns were also collected to complement the assessment of digital behaviours.
Socioeconomic and family context were characterized using parental educational level, classified according to the International Standard Classification of Education (ISCED), parental occupation based on the International Standard Classification of Occupations (ISCO), and the Family Affluence Scale (FAS), providing a comprehensive assessment of socioeconomic status. In the same questionnaire, they were asked for Tanner status to self-reporting using images as reference. A brief medical history was also requested.
Clinical and biological assessment
Anthropometric measurements and blood pressure are obtained during in-person visits. Height was measured using a portable stadiometer SECA 213. Body composition is assessed primarily by bioelectrical impedance analysis using the Tanita MC-580. For logistic reasons, only in participants from Zaragoza (the city from where the study is coordinated and with the DXA available) dual-energy X-ray absorptiometry (HOLOGIC Horizon DXA scan) is performed to obtain detailed body composition data. The waist-to-hip ratio was also obtained using the Ergonomic circumference measuring tape SECA201, as well as blood pressure measured twice within a 5-minute interval (if systolic or diastolic pressure differed by more than 5%, a third measurement was taken). To assess physical condition, manual dynamometry (Hand grip Takei 5001 Grip-A) and the longitudinal jump test were used, which evaluate the strength of the upper and lower limbs with 2 repetitions both measurements.
Fasting blood samples are collected in a sub-sample of participants to determine lipid profile, glycaemic markers and inflammatory biomarkers. The blood tests were performed in fasting status, first thing in the morning. In Zaragoza, these tests were carried out at the Lozano Blesa University Clinical Hospital, while in Huesca and Teruel, the samples were taken at their respective primary care health centers (Public health centres). Blood tests included: a) complete blood count: hemoglobin, hematocrit, red blood cells, mean corpuscular volume (MCV), white blood cells, monocytes, lymphocytes, eosinophils, basophils, neutrophils, platelets; b) biochemistry: glucose, urea, keratinine, ALT (SGPT), AST (SGOT), uric acid, total protein, insulin, and glycated hemoglobin; c) lipid profile: total cholesterol, HDL-c, LDL-c, triglycerides, Apo B100, Apo A1; d) inflammatory markers: C-reactive protein
(CRP), leptin, and interleukin 6 (IL-6). Biological samples from participants who provided additional consent are stored in the Aragón Biobank for future research purposes.
OUTCOMES
The primary outcome is cardiovascular health in adolescence, assessed using the Life’s Essential 8 score. Cardiovascular health will be assessed using the American Heart Association’s Life’s Essential 8 (LE8) framework, which integrates four health behaviours and four health factors. The behavioural components include diet quality, physical activity, nicotine exposure and sleep health. The health
factors comprise body mass index, blood lipids, blood glucose and blood pressure. Each component is scored on a continuous scale from 0 to 100 according to predefined criteria, with higher scores indicating better cardiovascular health. An overall LE8 score is calculated as the
unweighted mean of the eight individual components, providing a global measure
of cardiovascular health.
In the present study, diet quality will be derived from the food frequency questionnaire; physical activity from the IPAQ-A; nicotine exposure from self-reported smoking behaviour; and sleep health from questionnaire-based sleep duration and quality measures. Health factors will be assessed using anthropometric measurements (body mass index), blood pressure measurements, and biochemical markers obtained from fasting blood samples, including lipid profile and glycaemic indicators.
Secondary outcomes include its individual components, anthropometric and body composition indicators, blood pressure, physical fitness, biochemical markers and psychosocial health variables.
SAMPLE SIZE AND DATA STRUCTURE
The expected sample size for the current wave is approximately 300 adolescents from Aragón. The initial target sample size for the adolescent follow-up was higher; however, the final number of participants reflects the operational constraints inherent to longitudinal cohort studies conducted in
real-world settings. Recruitment was conducted over a limited time window, and participation in in-person assessments required additional logistical coordination across different provinces.
Despite this, the study retains its scientific value due to its longitudinal design, the availability of early-life data, and the depth of phenotyping achieved in adolescence. Although the sample size is moderate, it is comparable to other deeply phenotyped cohort studies and allows for robust analyses of cardiovascular health and its determinants.
Data availability varies across study modules:
- Questionnaire data: ~100%
- Body composition and Physical fitness: ~97%
- Blood samples: ~75%
- DXA: sub-sample (mainly Zaragoza, ~75%)
Although the sample size is moderate, the depth of phenotyping and the availability of longitudinal data from birth provide a unique opportunity to investigate life-course determinants of cardiovascular health.
Statistical Analysis
Descriptive analyses will be performed to characterize the study population at 16–17 years of age. Continuous variables will be summarized using appropriate measures and categorical variables as frequencies.
The Life’s Essential 8 score will be analysed both as a continuous variable and, when appropriate, using categorical classifications. Cross-sectional associations between cardiovascular health and lifestyle behaviours, body composition and psychosocial variables will be analysed using multivariable regression models, adjusting for relevant confounders.
Longitudinal analyses will examine the relationship between early-life factors collected in the CALINA cohort and cardiovascular health in adolescence.
Primary analyses of body composition will rely on anthropometric and bioimpedance-derived measures due to their broad availability. DXA-based analyses will be restricted to the sub-sample with available data.
Exploratory analyses may include identification of behavioural and psychosocial profiles using data-driven approaches and development of simplified models for cardiovascular risk screening.
Missing Data
Data completeness will be assessed across study modules, and differences between participants with and without optional assessments will be explored.
Multiple imputation may be considered for partially missing covariates or questionnaire-derived variables. However, DXA-derived measures and optional blood-based biomarkers will not be imputed and will be analysed within observed sub-samples.
Sensitivity analyses will be performed to assess the impact of missing data and potential selection bias.
Protocol references
1. Lloyd-Jones DM, Allen NB, Anderson CAM, Black T, Brewer LC, Foraker RE, Grandner MA, Lavretsky H, Perak AM, Sharma G, Rosamond W; American Heart Association. Life's Essential 8: Updating and Enhancing the American Heart Association's Construct of Cardiovascular Health: A Presidential Advisory From the American Heart Association. Circulation. 2022 Aug 2;146(5):e18-e43. doi: 10.1161/CIR.0000000000001078. Epub 2022 Jun 29. PMID: 35766027; PMCID: PMC10503546.
2.Ahrens W, Siani A, Adan R, De Henauw S, Eiben G, Gwozdz W, Hebestreit A, Hunsberger M, Kaprio J, Krogh V, Lissner L, Molnár D, Moreno LA, Page A, Picó C, Reisch L, Smith RM, Tornaritis M, Veidebaum T, Williams G, Pohlabeln H, Pigeot I; I.Family consortium. Cohort Profile: The transition from childhood to adolescence in European children-how I.Family extends the IDEFICS cohort. Int J Epidemiol. 2017 Oct 1;46(5):1394-1395j. doi: 10.1093/ije/dyw317. PMID: 28040744; PMCID: PMC5837508.
3.Ferrer-Santos P, Iglesia I, Muñiz-Pardos B, Miguel-Berges ML, Flores-Barrantes P, Moreno LA, Rodríguez-Martínez G. Moderate-to-Vigorous Physical Activity and Body Composition in Children from the Spanish Region of Aragon. Children (Basel). 2021 Apr 26;8(5):341. doi: 10.3390/children8050341. PMID: 33926063; PMCID: PMC8146711.
4.Goodman R. The Strengths and Difficulties Questionnaire: a research note. J Child Psychol Psychiatry. 1997 Jul;38(5):581-6. doi: 10.1111/j.1469-7610.1997.tb01545.x. PMID: 9255702.
5.Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 Well-Being Index: a systematic review of the literature. Psychother Psychosom. 2015;84(3):167-76. doi: 10.1159/000376585. Epub 2015 Mar 28. PMID: 25831962.
6. Xiao T, Zhu F, Wang D, Liu X, Xi SJ, Yu Y. Psychometric validation of the Perceived Stress Scale (PSS-10) among family caregivers of people with schizophrenia in China. BMJ Open. 2023 Nov 30;13(11):e076372. doi: 10.1136/bmjopen-2023-076372. PMID: 38035751; PMCID: PMC10689371.
7. Andreassen CS, Torsheim T, Brunborg GS, Pallesen S. Development of a Facebook Addiction Scale. Psychol Rep. 2012 Apr;110(2):501-17. doi: 10.2466/02.09.18.PR0.110.2.501-517. PMID: 22662404.
8. Hagströmer M, Bergman P, De Bourdeaudhuij I, Ortega FB, Ruiz JR, Manios Y, Rey-López JP, Phillipp K, von Berlepsch J, Sjöström M; HELENA Study Group. Concurrent validity of a modified version of the International Physical Activity Questionnaire (IPAQ-A) in European adolescents: The HELENA Study. Int J Obes (Lond). 2008 Nov;32 Suppl 5:S42-8. doi: 10.1038/ijo.2008.182. PMID: 19011653.
9. Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: the development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Soc Sci Med. 2008 Mar;66(6):1429-36. doi: 10.1016/j.socscimed.2007.11.024. Epub 2008 Jan 7. PMID: 18179852.
10. UNESCO Institute for Statistics. International Standard Classification of Education (ISCED). Montreal: UNESCO; 2012.
11.International Labour Organization. International Standard Classification of Occupations (ISCO-08). Geneva: ILO; 2012.
12.Wells JC, Fewtrell MS. Measuring body composition. Arch Dis Child. 2006 Jul;91(7):612-7. doi: 10.1136/adc.2005.085522. PMID: 16790722; PMCID: PMC2082845.
Acknowledgements
We acknowledge Instituto de Investigación Sanitaria de Aragón (IISA), University of Zaragoza (GENUD Research group), Hospital Clínico Lozano Blesa, primary care centres in Huesca and Teruel, and hospitals Obispo Polanco and San Jorge. We also thank all professionals and collaborators involved in the study, as well as the participating families.