Apr 26, 2025
Automated VMAT Planning for Short-Course Radiotherapy in Locally Advanced Rectal Cancer
- qiong zhou1,
- Liwen Qian1,
- Chong Shen1,
- Xinyan Bei1,
- Gaojie Liu1,
- Xiaonan Sun1
- 1Sir Run Run Shaw Hospital



Protocol Citation: qiong zhou, Liwen Qian, Chong Shen, Xinyan Bei, Gaojie Liu, Xiaonan Sun 2025. Automated VMAT Planning for Short-Course Radiotherapy in Locally Advanced Rectal Cancer. protocols.io https://dx.doi.org/10.17504/protocols.io.q26g7357qvwz/v1
License: This is an open access protocol distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Protocol status: Working
We use this protocol and it's working
Created: April 25, 2025
Last Modified: April 26, 2025
Protocol Integer ID: 157679
Keywords: auto-planning, SCRT, Dosimetry, plan quality, LARC, advanced rectal cancer this protocol, course radiotherapy, automated vmat planning for short, automated vmat planning, vmat plan generation, advanced rectal cancer, rectal cancer, raystation tp, dosimetric constraint, dose calculation, clinical data selection, automated plan, manual plan, comparing manual plan, monaco tps with automated plan, optimization procedure, contouring workflow, procedure, detailed optimization parameter
Abstract
This protocol outlines the clinical data selection, contouring workflow, VMAT plan generation, and optimization procedures comparing manual plans (MPs) using Monaco TPS with automated plans (APs) implemented on RayStation TPS for short-course radiotherapy (SCRT) in rectal cancer. It includes detailed optimization parameters, dosimetric constraints, dose calculation algorithms, and convergence criteria.
Guidelines
This retrospective study was based on CT imaging data obtained from an anonymized database of patients who had completed treatment, with no additional patient intervention or data acquisition involved.This study was approved by the Ethics Committee of Sir Run Run Shaw
Hospital, Zhejiang University School of Medicine (Approval No. 2024-2147-01)
and was conducted in accordance with the ethical standards of the Declaration
of Helsinki.
Materials
Equipment:Monaco V6.00.11 TPS ,RayStation 9A TPS
Elekta Infinity linear accelerator
Software:Python v2.7
Safety warnings
This study utilized anonymized, retrospective CT data. No hazardous materials, biological agents, or high-risk procedures were involved.
1. Patient Cohort and Data AcquisitionInclusion
Criteria: Rectal adenocarcinoma, clinical stage T3a–T4a;Received neoadjuvant SCRT (25 Gy/5 fractions);Underwent prone-position CT simulation (3-mm slice thickness)
Exclusion Criteria:History of long-course radiotherapy (LCRT);Evidence of metastatic disease at treatment
Cohort Description:
Total: 30 patients
Median age: 61 years
Gender: 77% male
Ethics Statement:
Approved by the Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang
University (No. 2024-2147-01)
Data were de-identified and retrospectively collected between April–July 2024
Simulation and ContouringSimulation:
Position: Prone
CT Scan: 3-mm slice thickness
Immobilization: Standard pelvic immobilization device
Contouring:Performed by a single experienced radiation oncologist
Followed institutional and published consensus guidelines
Target Volumes:GTV: Gross tumor volume;CTV: Includes mesorectum, presacral, and internal iliac nodes;PTV: CTV + 3 mm uniform margin
Organs-at-Risk (OARs): Small bowel, Bladder,Bilateral femoral heads, Pelvic marrow
Planning Constraints and Clinical Goals
PTV Goals:
- V25Gy ≥ 95%
- Dmax < 110% (27.5 Gy)
OAR Dose Constraints:
- Small bowel: V10Gy < 180–200 cc, V18Gy < 110 cc, V23Gy < 85 cc
- Bladder: V25Gy < 5%, V21Gy < 15%
- Femoral heads: V12.5Gy < 11%
- Pelvic marrow: Minimize dose; avoid hotspots
Manual Planning
Platform:
- Monaco v6.00.11
- Elekta Infinity linac
- Dose rate: 1400 MU/min
- Beam energy: 6 MV FFF
- Dose grid: 0.25 cm
- Delivery technique: Dual-arc VMAT (Arc1: 204°→156°, Arc2: 156°→204°)
- Plan uncertainty: 0.7%
Dose Calculation:
- XVMC algorithm (based on VMC)
- Fast stochastic modeling with energy cutoffs and transport approximations
Planning Personnel:
- Dosimetrist with >5 years of experience
- Clinically approved by senior physicians
Auto-Planning
Platform:
- RayStation 9A
- Python scripting (v2.7)
- Same machine specs and beam settings as MP
Dose Calculation:
- Monte Carlo (EGSnrc-based)
- GPU-accelerated computation
Optimization Method:
- DMPO (Direct Machine Parameter Optimization)
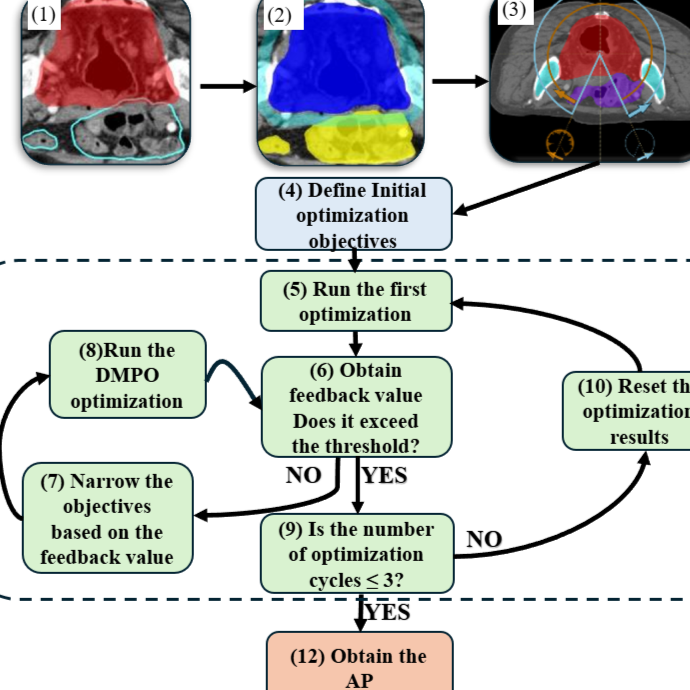
Auto-Planning Workflow Script Logic:
Structured into 5 steps:
Step 1: Initial Plan Creation
- Create beams, auxiliary structures, and define loose optimization objectives
- Add dose objectives for PTV and OARs
Step 2: First Pass Optimization
- Run 30-step flux optimization (fluence map optimization)
- Evaluate and adapt objectives according to dose feedback
Step 3: Evaluation and Tightening
- Analyze convergence values from feedback
- If not meeting thresholds (e.g., objective value > 4e-4), tighten constraints
- Evaluate target coverage and OAR sparing
Step 4: Iterative Cycles
- Up to 3 optimization cycles (100 iterations/cycle)
- Normalization to prescribed dose
Step 5: Termination and Restart Criteria
- Terminate optimization if convergence is achieved or thresholds are met
- If cycles exceed 3 without convergence, reset plan and restart to reduce complexity
Note:
- AP plans were for research only and not delivered clinically
- Fig. 1 (in main manuscript) shows the full automation workflow
Data Management and Analysis
- Plans stored in DICOM-RT format
- Dosimetric parameters (e.g., CI, HI, MU, OAR doses) extracted using in-house Python tools
- Statistical comparisons between MP and AP conducted using paired tests
CitationPlease
cite the main paper (once published) or contact the corresponding author for
access to the automation script or patient dataset.