Jun 29, 2026
A standardized protocol for establishing minimally invasive mouse models of jaw osteonecrosis: bisphosphonate-related and radiation-induced models
- Zhangfan Ding1,
- Junyu Chen1,
- Anjali Kusumbe2
- 1State Key Laboratory of Oral Diseases, National Center for Stomatology, National Clinical Research Center for Oral Diseases, West China Hospital of Stomatology, Sichuan University, Chengdu 610041, China. Tissue and Tumor Microenvironments Lab, Cancer Discovery and Regenerative Medicine Program, Lee Kong Chian School of Medicine, Nanyang Technological University, 636921 Singapore;
- 2Tissue and Tumor Microenvironments Lab, Cancer Discovery and Regenerative Medicine Program, Lee Kong Chian School of Medicine, Nanyang Technological University, 636921 Singapore. Multidisciplinary Institute of Ageing (MIA-Portugal), University of Coimbra, Coimbra 3004-504, Portugal
- Anjali Kusumbe: Corresponding author;
- KUSUMBE LAB



Protocol Citation: Zhangfan Ding, Junyu Chen, Anjali Kusumbe 2026. A standardized protocol for establishing minimally invasive mouse models of jaw osteonecrosis: bisphosphonate-related and radiation-induced models. protocols.io https://dx.doi.org/10.17504/protocols.io.n2bvj5xpwgk5/v1
License: This is an open access protocol distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Protocol status: Working
We use this protocol and it's working
Created: June 29, 2026
Last Modified: June 29, 2026
Protocol Integer ID: 319963
Keywords: osteomyelitis, mouse model, bisphosphonates, radiation-induced injury, mandible
Abstract
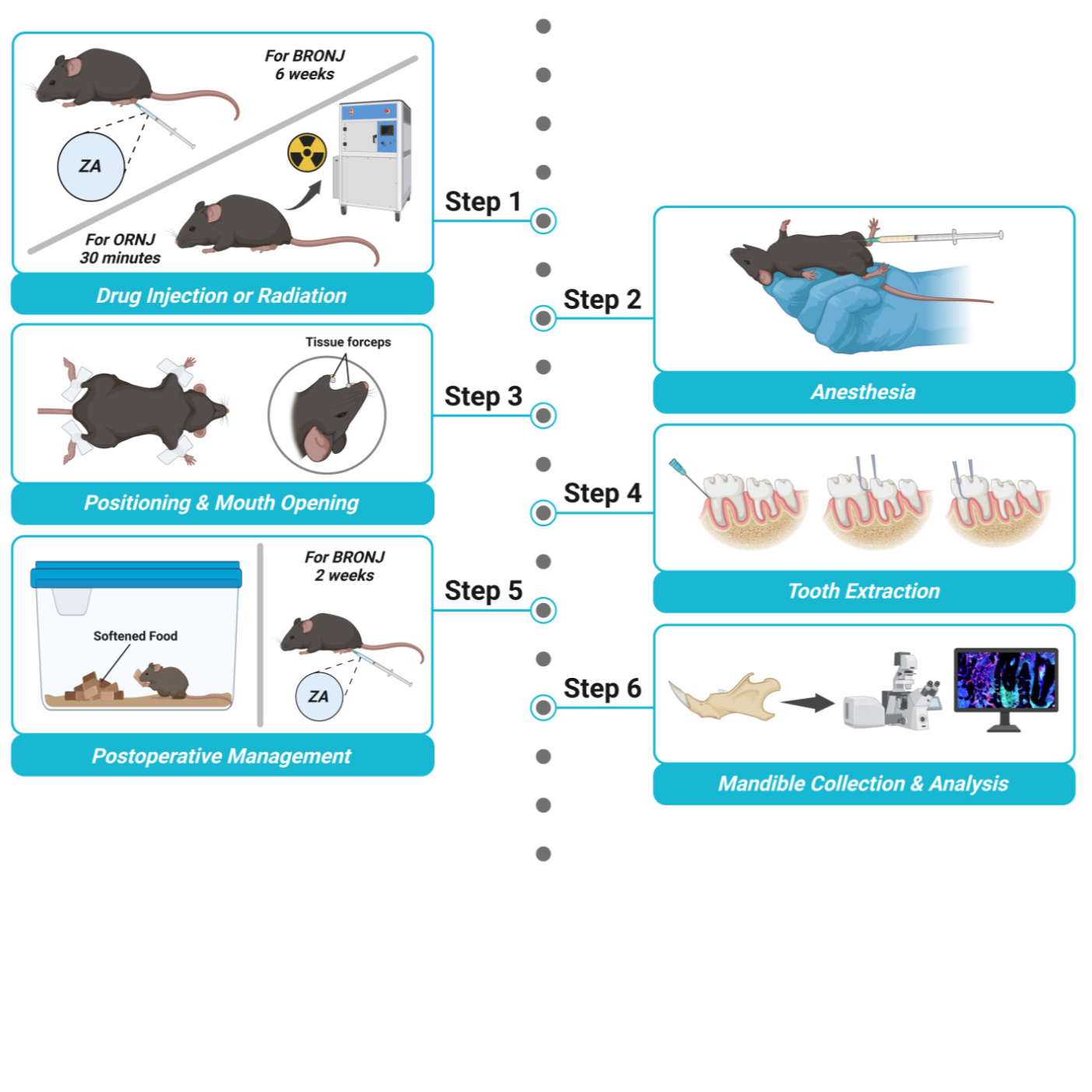
This protocol describes a standardized and reproducible minimally invasive method for establishing mouse models of bisphosphonate-related osteonecrosis of the jaw (BRONJ) and osteoradionecrosis of the jaw (ORNJ) in adult male C57BL/6 mice. The procedure integrates a unified minimally traumatic oral surgical approach with distinct injury induction strategies for each condition. In BRONJ, systemic zoledronic acid administration is combined with mandibular first molar extraction using tape-assisted mouth opening and bent micro-forceps to reduce soft tissue injury and procedural variability. In ORNJ, a customized lead shielding system enables precise, noninvasive, mandible-targeted irradiation, ensuring reproducible bone injury with minimized off-target effects. Together, these models provide a consistent minimally invasive framework for studying jaw osteonecrosis across different etiologies, supporting downstream micro-CT, histological, and immunofluorescence analyses, and enabling investigations of disease mechanisms, bone repair, and therapeutic interventions.
Image Attribution
Figure 1. The establishment and validation of the mouse ORNJ model
Figure 2. The surgical preparation and positioning of the mouse before tooth extraction
Figure 3. Histological analysis of the BRONJ and ORNJ compared with control
Troubleshooting
Problem
Inadequate radiation injury (step “Animal preparation”, 5-6).
Solution
Ensure sufficient anesthesia to avoid changed location of mouse mandible. Adjust the chamber lid to expose the mandible to radiation area.
Problem
Inadequate anesthesia (step “Animal preparation”, 12).
Solution
Inject the reagents strictly and slowly according to the dosage provided by the reagent manufacturer and the actual weight of the mice. Pay attention to the position of the mouse during the injection and the depth of the needle insertion. Do not make large movements that may cause bleeding in the abdominal cavity of the mouse.
Problem
Excessive bleeding during surgery (step “Tooth extraction”, 16-18).
Solution
During the operation, be careful not to damage the soft tissues such as the gums, tongue, and mucosa with sharp metal instruments. The forceps used to open the mouth can be separated by several cotton balls and the mouse's tongue to prevent mechanical damage. Be careful to insert the micro-forceps into the root bifurcation area gently and do not clamp the gums.
Problem
Crown fracture (step “Tooth extraction”, 18).
Solution
Avoid using sudden and excessive external force. Instead, apply controlled and gradual force. Find a stable fulcrum and you can appropriately generate force through the movements of your wrist and arm.
Problem
Weight loss (step “Postoperative care”, 24).
Solution
Provide appropriate soft food. If approved by the IACUC, consider using analgesic (buprenorphine 0.05-0.1 mg/kg SC). If the condition persists, humane endpoint should be applied to the mice.
Problem
Death after radiation and tooth extraction (step “Preoperative management”, 6; “Postoperative care”, 24).
Solution
Avoid excessive exposure to radiation and additional injury.Check the setting of irradiator to esure proper radiation dose. Provide softened food after radiation and tooth extraction.
For BRONJ
House mice (8-12 weeks old male C57BL/6J) in standard cages with a 12 h light/dark cycle and ad libitum access to food and water.
Weighing each mouse. The mice are injected intraperitoneally with the prepared solution at a dose of 200 µg/kg of ZA, three times a week.
For ORNJ
House mice (8-12 weeks old male C57BL/6J) in standard cages with a 12 h light/dark cycle and ad libitum access to food and water.
Weighing each mouse. The mice are injected intraperitoneally with the prepared solution at a dose of 0.2 mL/10g of tribromoethyl alcohol (Avertin).
Place the mouse in the customized lead chamber in a supine position. Close the lid and leave a square opening to expose only the mandible. Adjust the area of the gap according to the size of the mandible. The chamber can accommodate 4 mice at a time.
Set the single radiation dose to 16 Gy and start radiation. Take out the mice from the chamber and transfer them to the cage.
Feed the mice in standard cages with a 12 h light/dark cycle and ad libitum access to food and water.
Before the tooth extraction surgery, prepare the following instruments in advance and place them in the high-pressure sterilization and disinfection surgical instruments.
Micro-forceps, the tip of which should be bent beforehand, to grasp the bifurcation when extracting the mandibular first molar (M1) and loosen the tooth before extraction.
B. Blunt tissue forceps, one of which used as a buccal retractor when exposing the mandibular molar area and another used as a mouth opener.
Disposable syringe needles (at least 2 per mouse) to fix the mouth opener and separate the gingiva.
Sterile cotton balls used for stopping bleeding and cleaning the surgical site.
Ophthalmic scissors to cut tape.
Use disposable surgical drapes to set up the surgical table for mice. Disinfect the surgical table (a foam board, 32×22×2.5cm), injection syringe, tape and heating pad (37 °C, 18×10 cm) with 75% ethanol.
Disinfect the surgical table with 75% ethanol. Put on the sterile disposable surgical gown, gloves, mask, and head cover. Place the sterilized instruments and materials that have been wiped with 75% ethanol on the disinfected surgical table.
Animal preparation
Weighing the mice.
Anesthetize the mice using 0.2ml/10g Avertin intraperitoneally.
Place the mouse on the surgical table and position it in a supine position. Secure the limbs with tape. Use one of the tissue forceps to open the mouth through the upper and lower incisors, and fix the tissue forceps to the surgical table by the disposable syringe needles and the tape.
Tooth extraction
Use blunt-tipped forceps to gently open the mouth and expose the area of the left lower molars.
Use sterile cotton balls with normal saline to clean the tooth surfaces and gum grooves, to remove debris from the mouth. Use sterile cotton balls with povidone-iodine solution to gently wipe the left M1 area for about 5-10 seconds.
One hand pulls the left buccal mucosa of the mouse, and uses disposable syringe needles to separate the gingiva of left M1.
Close the tips of the bent micro-forceps to pass through the gap between the first and second molars on the lower jaw. While rotating along the long axis of the instrument, forcefully close the tip of the micro-forceps to loosen left M1.
Use the bent micro-forceps to firmly grasp the root bifurcation of left M1, apply force along the long axis of the tooth, and perform lateral movements in both the buccal and palatal directions. During the shaking process, apply vertical force towards the occlusal surface to dislodge the tooth and complete the extraction.
Check whether the tooth root is intact, and whether there are any fragments of alveolar bone or large masses of soft tissue attached to it. Clean the surgical area with normal saline.
Following the above steps, remove the right M1 similarly.
Postoperative care
After the surgery, gently remove the mouse from the fixed surgical plate. Drop a drop of normal saline on the tip of the mouse's tongue to moisten its mouth.
Place the mouse on the heating pad and keep it in a prone position. The head should be tilted to one side to prevent liquid from entering the mouse's respiratory tract.
Maintain this position until the mouse regains consciousness. Continuously observe whether the mouse has regained consciousness, whether there is breathing difficulty, and whether there is continuous bleeding in the surgical area.
Transfer the animals to clean cages and feed the mice in standard cages with a 12 h light/dark cycle and ad libitum access to food and water. Provide fresh and softened food.
Postoperative drug injection (Only For BRONJ)
After the surgery, continuous medication injection is required for 2 other weeks, with the prepared solution at a dose of 200 µg/kg of ZA, three times a week as before.
Tissue collection
After the mice complete 8 weeks of drug injection, euthanize the mouse using carbon dioxide (CO2) inhalation until they stopped moving. Use cervical dislocation to ensure the mice totally death.
The mandibles of the mice were collected and the soft tissues on the bones were scraped off.
Immerse the mandibles of the mice in 4% Paraformaldehyde solution at 4°C for 3 hours. Rinse 3 times with PBS for 5 minutes each. Afterwards, store the samples in PBS at 4°C.
Micro-CT analysis
Remove the mandibles from the PBS and place it in the micro-CT scanner with preset parameters. This protocol uses a 34mm diameter sample tube for scanning, with Voxel size 10.0 μm, FOV 35.36 mm, Image matrix 3400×3400×775, Slices 775, Voltage 55 kVp, Intensity 145 μA. Return the scanned samples in PBS for storage.
Reconstruct 3D images using the manufacturer's software (DataViewer and CTvox). Lower and upper gray threshold values set to 130 and 255.
Histology or immunofluorescence analysis
Decalcify in 10% EDTA (pH 7.4) for 5 days at 4 °C, changing the solution every day. Wash the samples 3 times using PBS for 10 minutes each.
Process the samples by the automatic tissue processor treated with ethanol of different concentrations (70%, 80%, 95% and 100%) first and then xylene.
Insert the maxilla into the embedding mold and confirm that the sagittal plane is correct. Quickly inject 60 °C paraffin and gently press the specimen to prevent air bubbles. Cool at room temperature until complete solidification.
Sectioning. The thickness of the section is 3 μm. The section is attached to a positively charged adhesive slide. This protocol uses H&E staining to evaluate the modeling effects of the model of BRONJ in mice.
Place and scan in the digital slide scanner.
The samples are subjected to dehydration treatment with 20% sucrose and 2% polyvinylpyrrolidone in 4 °C for 24 hours. Then embed the samples 20% sucrose, 2% polyvinylpyrrolidone and 8% gelatin. Cut the samples into 80 μm thick sections using a low-profile blade on the cryostat and dry in air before being stored in a freezer in -20 °C.
Perform permeabilization with Triton X-100, block with 5% horse serum, and conduct immunostaining with antibody solution. Add the nuclear marker DAPI to the secondary antibody solution for staining.
Place and scan in the spinning disk confocal microscope.
The images captured on the digital slide scanner are processed using OlyVIA. The images captured on the spinning disk confocal microscope are processed and reconstructed using Imaris and Imaris File Converter. Adobe Illustrator software is used for image processing and analysis.
Protocol references
1. Wang, W.Y., Chen, L.H., Ma, W.J., and You, R.X. (2023). Drug efficacy and safety of denosumab, teriparatide, zoledronic acid, and ibandronic acid for the treatment of postmenopausal osteoporosis: a network meta-analysis of randomized controlled trials. Eur Rev Med Pharmacol Sci 27, 8253-8268. 10.26355/eurrev_202309_33586.
2. Lund, T., Gundesen, M.T., Juul Vangsted, A., Helleberg, C., Haukås, E., Silkjær, T., Asmussen, J.T., Manuela Teodorescu, E., Amdi Jensen, B., Schmidt Slørdahl, T., et al. (2024). In multiple myeloma, monthly treatment with zoledronic acid beyond two years offers sustained protection against progressive bone disease. Blood Cancer J 14, 65. 10.1038/s41408-024-01046-2.
3. Annamalai, S., Kamalakaran, A., Jayaraman, B., Selvakumar, A., and Kulkarni, H.S. (2025). Multidisciplinary approach for medication-related osteonecrosis of the jaws: a case report and literature review. Arch Craniofac Surg 26, 70-75. 10.7181/acfs.2024.0091.
4. Martins, L.H.I., Ferreira, D.C., Silva, M.T., Motta, R.H.L., Franquez, R.T., and Bergamaschi, C.C. (2023). Frequency of osteonecrosis in bisphosphonate users submitted to dental procedures: A systematic review. Oral Dis 29, 75-99. 10.1111/odi.14003.
5. Topkan, E., Kucuk, A., Somay, E., Yilmaz, B., Pehlivan, B., and Selek, U. (2023). Review of Osteoradionecrosis of the Jaw: Radiotherapy Modality, Technique, and Dose as Risk Factors. J Clin Med 12. 10.3390/jcm12083025.
6. Jelin-Uhlig, S., Weigel, M., Ott, B., Imirzalioglu, C., Howaldt, H.P., Böttger, S., and Hain, T. (2024). Bisphosphonate-Related Osteonecrosis of the Jaw and Oral Microbiome: Clinical Risk Factors, Pathophysiology and Treatment Options. Int J Mol Sci 25. 10.3390/ijms25158053.
7. Filho, A.M., Laversanne, M., Ferlay, J., Colombet, M., Piñeros, M., Znaor, A., Parkin, D.M., Soerjomataram, I., and Bray, F. (2025). The GLOBOCAN 2022 cancer estimates: Data sources, methods, and a snapshot of the cancer burden worldwide. Int J Cancer 156, 1336-1346. 10.1002/ijc.35278.
8. Rogers, S.N., D'Souza, J.J., Lowe, D., and Kanatas, A. (2015). Longitudinal evaluation of health-related quality of life after osteoradionecrosis of the mandible. Br J Oral Maxillofac Surg 53, 854-857. 10.1016/j.bjoms.2015.07.008.
9. de Almeida-Silva, L.A., Lupp, J.D.S., Sobral-Silva, L.A., Dos Santos, L.A.R., Marques, T.O., da Silva, D.B.R., Caneppele, T.M.F., and Bianchi-de-Moraes, M. (2024). The incidence of osteoradionecrosis of the jaws in oral cavity cancer patients treated with intensity-modulated radiotherapy: a systematic review and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol 138, 66-78. 10.1016/j.oooo.2024.04.008.
Acknowledgements
A.P.K. is supported by Ministry of Education (MOE) Singapore: Academic
Research Funds (#024983-00001 and #025277-00026), European Research
Council (StG: metaNiche, 805201), and European Union’s Horizon 2020 (no.
857524).